Focal nodular hyperplasia revealed with new imaging modalities [July 2025]
October 15, 2025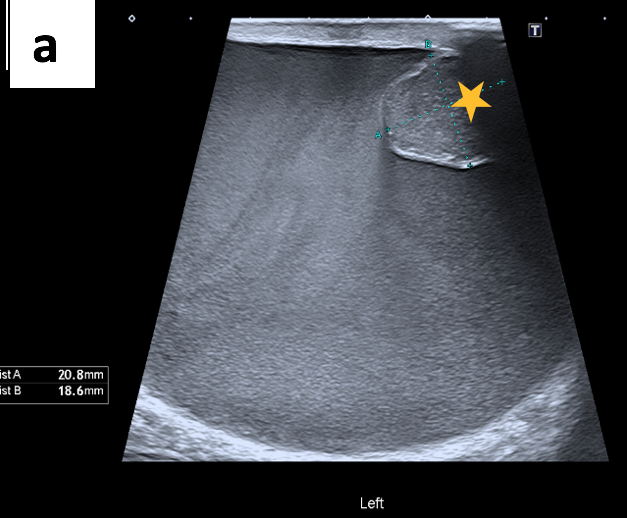
Rare Multinodular Epithelioid Malignant Mesothelioma of the Tunica Vaginalis [September 2025]
November 26, 2025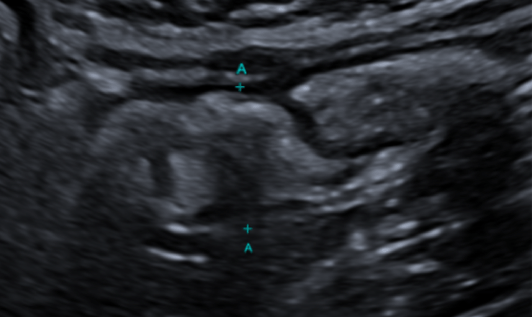
SUBMIT YOUR CASE
EFSUMB invites submission of interesting cases for the website section 'Case of the Month'. All CoM submissions are eligible for selection for free registration at the next Euroson congress. Two cases that receive the most 'likes' in a year will receive free registration for the next EUROSON congress and the third most liked liked case will receive a cash prize of 100 EUR.
Incidental finding of an appendiceal mucocele
Authors:
Aida J. Raigoso, Ana Poza, Soledad Vera, Karina Rodriguez, Nerea Alava, Ana Ginon, Daniel Pelaez, Valentín Moratalla, Eva Manuela Pena, Huáscar Galindo.
Gregorio Marañón Hospital, Madrid, Spain.
1Clinical History
Male patient, aged 42, referred for ultrasound assessment to evaluate the progression of long-standing penetrating ileal Crohn’s disease.
On examination, mural thickening of the terminal ileum is observed, extending 6 cm in the craniocaudal direction, with a maximum mural thickness of 4 mm in the more distal terminal ileum. The layered pattern is preserved, with no evidence of ulceration or adipose proliferation. No free fluid is present. The Doppler study shows grade 0-1 activity on a scale of 0 to 3, and after intravenous administration of contrast (Sonovue 1.5 cc), no signs of inflammatory activity are demonstrated.
On examination, mural thickening of the terminal ileum is observed, extending 6 cm in the craniocaudal direction, with a maximum mural thickness of 4 mm in the more distal terminal ileum. The layered pattern is preserved, with no evidence of ulceration or adipose proliferation. No free fluid is present. The Doppler study shows grade 0-1 activity on a scale of 0 to 3, and after intravenous administration of contrast (Sonovue 1.5 cc), no signs of inflammatory activity are demonstrated.
2Image Findings
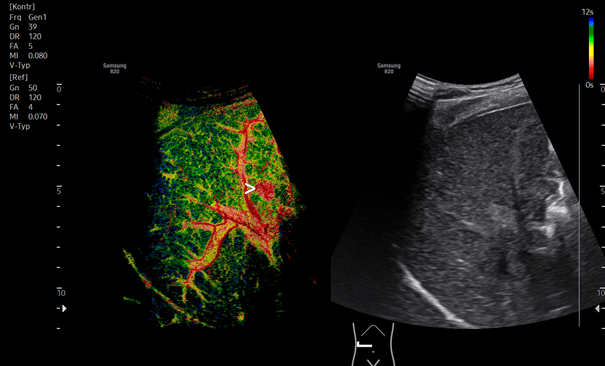
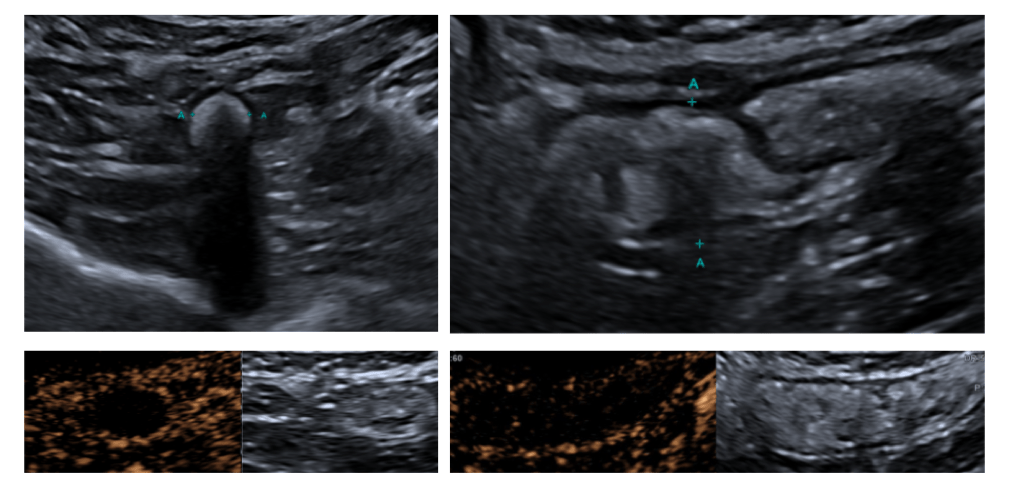
B-mode ultrasound and Contrast-enhanced ultrasound (CEUS)
An enlarged appendix is identified, measuring 15 mm in diameter and 4.8 cm in length, with a distal appendicolith measuring 8 mm (yellow arrow). After IV contrast administration, there is mural enhancement (2 mm) (Blue arrow) with no intraluminal contrast opacification. These findings suggest an appendiceal mucocele (mucinous neoplasm). No signs of complication are observed. (Fig. 1)
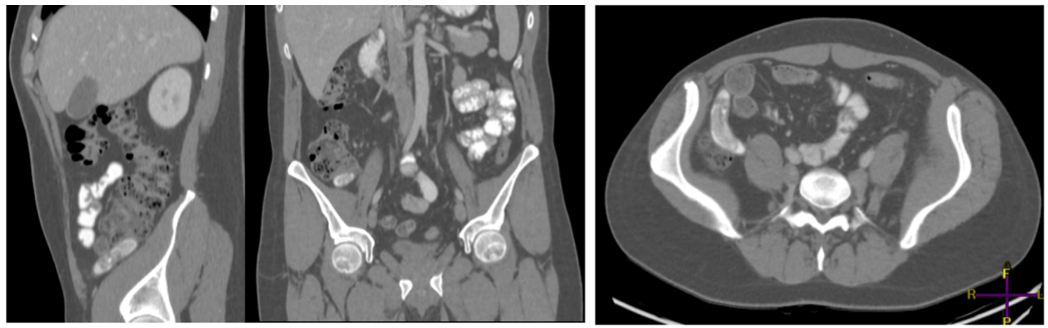
CT with intravenous contrast: Confirmed dilatation of the vermiform appendix (Red arrow), showing heterogeneous hyperdense content with layering and measuring 56 x 16 mm. It contains hyperdense material and calcifications (appendicoliths), with no evidence of local complication. This suggests an appendiceal tumor, likely mucinous in origin.
No free fluid or peritoneal implants are detected. Mild mural thickening (3 mm) of the terminal ileum is observed, with no associated local inflammatory changes to indicate active inflammation (Fig 2).
CT with intravenous contrast: Confirmed dilatation of the vermiform appendix (Red arrow), showing heterogeneous hyperdense content with layering and measuring 56 x 16 mm. It contains hyperdense material and calcifications (appendicoliths), with no evidence of local complication. This suggests an appendiceal tumor, likely mucinous in origin.
No free fluid or peritoneal implants are detected. Mild mural thickening (3 mm) of the terminal ileum is observed, with no associated local inflammatory changes to indicate active inflammation (Fig 2).
3Surgery
The appendiceal base is identified, and the mesoappendix is dissected with clips applied. The appendix is then transected, hemostasis is confirmed, and the surgical site is closed. The specimen is sent for pathology analysis.
4Diagnosis
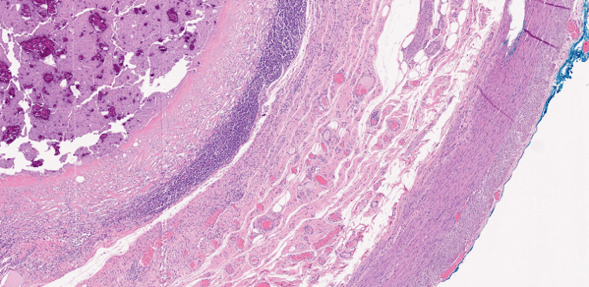
The appendiceal lumen is swollen and filled with mucinous material that contains food debris and calcifications. The wall appears flattened, with loss of the epithelial lining. The submucosa shows fibrosis and moderate lymphocytic infiltration. The muscularis propria is heavily infiltrated with inflammatory cells. Mucinous material is not present within the appendiceal wall, and no epithelial dysplasia is observed (Fig 3.)
5Teaching Points
● Echography: Appearance: Cystic, tubular, or oval structure in the right iliac fossa, well-defined with a wall. Non-compressible, fixed structure. May show echogenic intraluminal material. Sometimes it exhibits shadows due to mural calcifications.
● CT scan: Useful for diagnosis and staging. Well-encapsulated, low-attenuation cystic mass with calcifications in less than 50% of cases.
● Treatment: If it's a benign appendectomy, then no further action needed. Suspicion of malignancy or involvement of the base or cecum requires a right hemicolectomy.
● CT scan: Useful for diagnosis and staging. Well-encapsulated, low-attenuation cystic mass with calcifications in less than 50% of cases.
● Treatment: If it's a benign appendectomy, then no further action needed. Suspicion of malignancy or involvement of the base or cecum requires a right hemicolectomy.
6References
1. Rumack CM, Wilson SR, Charboneu JW. Diagnóstico por ecografía. 2º edición. Ed. Marban. 1999.
2. Pickhardt PJ, Levy AD, Rohrmann CA Jr, Kende AI, Maj. Primary neoplasm of the appendix: Radiologic spectrum of disease with pathologic correlation. RadioGraphics. 2003; 23:645-662.
3. Madwed D, Mindelzun R, Jeffrey RB Jr. Mucocele of the appendix: Imaging findings. AJR. 1992; 159:69-72.
4. Kim SH, Lim Hk, Lee WJ, Lim JH, Byun JY. Mucocele of the appendix: ultrasonographic and CT findings. Abdom Imaging. 1998;23:292-296.
5. Sasaki K, Ishida H, Komatsuda T, Suzuki T, Konno K, Ohtaka M et al. Appendiceal mucocele: sonographic findings. Abdom Imaging. 2003;28:15-18.
2. Pickhardt PJ, Levy AD, Rohrmann CA Jr, Kende AI, Maj. Primary neoplasm of the appendix: Radiologic spectrum of disease with pathologic correlation. RadioGraphics. 2003; 23:645-662.
3. Madwed D, Mindelzun R, Jeffrey RB Jr. Mucocele of the appendix: Imaging findings. AJR. 1992; 159:69-72.
4. Kim SH, Lim Hk, Lee WJ, Lim JH, Byun JY. Mucocele of the appendix: ultrasonographic and CT findings. Abdom Imaging. 1998;23:292-296.
5. Sasaki K, Ishida H, Komatsuda T, Suzuki T, Konno K, Ohtaka M et al. Appendiceal mucocele: sonographic findings. Abdom Imaging. 2003;28:15-18.

{kind=link}