Vulnerable Plaque in Focus: A Multimodal Ultrasound Case Study with Triplex, High-Resolution Flow, and 3D Imaging [November 2025]
December 15, 2025
Student Image Challenge 108
February 2, 2026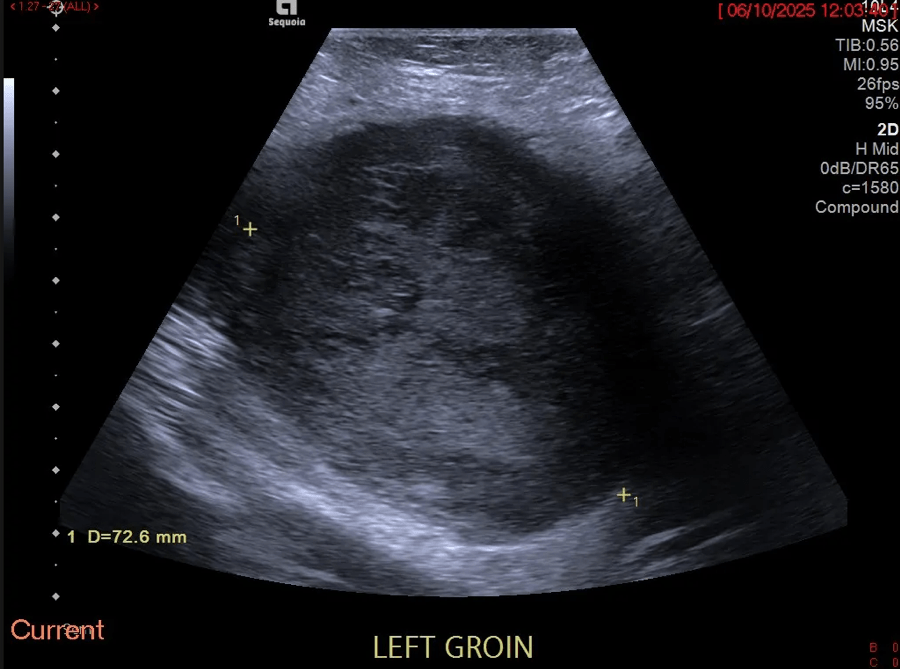
SUBMIT YOUR CASE
EFSUMB invites submission of interesting cases for the website section 'Case of the Month'. All CoM submissions are eligible for selection for free registration at the next Euroson congress. The EFSUMB Publications Committee will review all Best Case of the Month submissions at the end of March 2026. Two cases that receive the most 'likes' over a period from the last congress to March 2026 and judged on a range of factors, including scientific value, will receive free registration for the next EUROSON congress and the third case will receive a cash prize of 100 EUR.
Beyond the visible borders: imaging clues in an infiltrative subcutaneous tumour
Authors:
Dr Neil Limaye [1] neil.limaye3@nhs.net, Dr Hannah Masraf [1], Dr Henry Conchie [2], Professor Adrian Lim [1]Affiliation:
[1] Imperial College Healthcare NHS Trust[2] Chelsea & Westminster Hospital NHS Foundation Trust








1Clinical History
A 65-year-old patient with a history of radiotherapy-treated cervical cancer presented to the emergency department with a two-week history of a rapidly growing, painful left groin lump.
Physical examination revealed a fixed, palpable 7-8 cm soft tissue lump in the left medial inguinal region. The lab results demonstrated a raised CRP of 58.3 mg/L. The WCC (7.4 x 10^9/L) and the remainder of the blood was in normal ranges. The clinical team‚ working differential was either an abscess or a haematoma.
Physical examination revealed a fixed, palpable 7-8 cm soft tissue lump in the left medial inguinal region. The lab results demonstrated a raised CRP of 58.3 mg/L. The WCC (7.4 x 10^9/L) and the remainder of the blood was in normal ranges. The clinical team‚ working differential was either an abscess or a haematoma.
2Image Findings
Fig.01.Transverse B-mode extended field of view imaging demonstrates a 7.2 cm well-circumscribed left groin lesion with heterogenous echo texture and increased echogenicity.
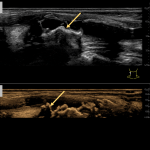
Fig.02. Transverse power Doppler extended field of view imaging shows marked peripheral and intra-lesional vascularity.
Fig. 03. Transverse pulse-wave Doppler imaging, targeted on an intra-lesional vessel, demonstrates arterial flow. The Doppler gain was increased, and the scale was reduced to maximise vascular signal from the central portions of the tumour, thereby producing an image with increased noise.
Fig.04. Ultrasound-guided core biopsy of the described left medial groin mass using B-mode extended field of view imaging.
Fig.05. Contrast-enhanced portal-venous phase axial CT of the abdomen and pelvis imaging demonstrates a heterogenous, peripherally-enhancing, mixed density lesion with adjacent inflammatory fat stranding and lateral displacement of the femoral vessels.
Fig.06. MRI Pelvis with T2-weighted PD fat-suppressed sequences again shows a large, heterogenous intermuscular mass in the medial compartment of the left upper thigh with associated mass effect and perilesional oedema.
Fig.07. MRI Pelvis with post-Gadolinium enhanced T2-weighted sequences. Post-contrast images reveal marked circumferential enhancement of the lesion's nodular soft-tissue components. There is a large central region of high signal intensity consistent with intra-tumoural necrosis.
Fig.08. Post-contrast T2-weighted MRI Pelvis with post-Gadolinium enhanced T2w sequences. Post-contrast images reveal marked circumferential enhancement of the lesion's nodular soft-tissue components. There is a large central region of high signal intensity consistent with intra-tumoural necrosis.
Fig.02. Transverse power Doppler extended field of view imaging shows marked peripheral and intra-lesional vascularity.
Fig. 03. Transverse pulse-wave Doppler imaging, targeted on an intra-lesional vessel, demonstrates arterial flow. The Doppler gain was increased, and the scale was reduced to maximise vascular signal from the central portions of the tumour, thereby producing an image with increased noise.
Fig.04. Ultrasound-guided core biopsy of the described left medial groin mass using B-mode extended field of view imaging.
Fig.05. Contrast-enhanced portal-venous phase axial CT of the abdomen and pelvis imaging demonstrates a heterogenous, peripherally-enhancing, mixed density lesion with adjacent inflammatory fat stranding and lateral displacement of the femoral vessels.
Fig.06. MRI Pelvis with T2-weighted PD fat-suppressed sequences again shows a large, heterogenous intermuscular mass in the medial compartment of the left upper thigh with associated mass effect and perilesional oedema.
Fig.07. MRI Pelvis with post-Gadolinium enhanced T2-weighted sequences. Post-contrast images reveal marked circumferential enhancement of the lesion's nodular soft-tissue components. There is a large central region of high signal intensity consistent with intra-tumoural necrosis.
Fig.08. Post-contrast T2-weighted MRI Pelvis with post-Gadolinium enhanced T2w sequences. Post-contrast images reveal marked circumferential enhancement of the lesion's nodular soft-tissue components. There is a large central region of high signal intensity consistent with intra-tumoural necrosis.
3Diagnosis
The constellation of imaging features on CT, ultrasound, and MRI was suspicious for a malignant soft-tissue lesion. The clinical working diagnoses included abscess, haematoma or metastatic lymph node from prior cervical cancer.
The patient was referred to a tertiary unit and underwent ultrasound-guided biopsy. The histopathology demonstrated an intramuscular myxoid sarcoma, favouring myxofibrosarcoma (MFS). The patient was referred for radiotherapy & definitive surgical management.
The patient was referred to a tertiary unit and underwent ultrasound-guided biopsy. The histopathology demonstrated an intramuscular myxoid sarcoma, favouring myxofibrosarcoma (MFS). The patient was referred for radiotherapy & definitive surgical management.
4Discussion
Lesion appearances, such as MFS, can be challenging. Ultrasound is a useful adjunct in assessment and differentiation of consistency, vascularity and compressibility. An ultrasound was performed using multi-frequency probes with M-mode and Doppler. The US demonstrated a 7.2cm heterogeneous vascular primary soft tissue tumour rather than an abnormal infiltrated lymph node (Figure 1-3).
Disorganised vascular patterns with abnormal morphology and flow characteristics are recognised as markers of malignancy. The US alone may underestimate deep extension or infiltrative margins, such as in MFS.
Disorganised vascular patterns with abnormal morphology and flow characteristics are recognised as markers of malignancy. The US alone may underestimate deep extension or infiltrative margins, such as in MFS.
5Learning Points
Learning Point 1: This case has demonstrated the essential role of multi-modality imaging in the early characterisation of complex soft tissue lesions such as MFS, helping differentiate malignant lesions from infective or inflammatory lesions
Learning Point 2: A comprehensive ultrasound assessment, combined with a focused clinical history and examination at the time of sonographic assessment, is essential in the initial assessment of complex soft tissue lesions. This is supported by the 2024 BMUS assessment of soft tissue lesion guidelines. Suspicious features of malignant soft tissue lesions, such as MFS, including rapid growth, marked intra-lesion vascularity, and a heterogeneous echotexture, were demonstrated in this case. They should prompt further investigation and onward referral.
Learning Point 3: While ultrasound is valuable for evaluating suspicious features of soft tissue lesions, gadolinium-enhanced MRI remains the gold standard for evaluating tumour extent and infiltrative spread. The tail sign of fascial spread was demonstrated in this case and is a key diagnostic sign, before formal histopathology confirmation (Figure 4-7).
Learning Point 2: A comprehensive ultrasound assessment, combined with a focused clinical history and examination at the time of sonographic assessment, is essential in the initial assessment of complex soft tissue lesions. This is supported by the 2024 BMUS assessment of soft tissue lesion guidelines. Suspicious features of malignant soft tissue lesions, such as MFS, including rapid growth, marked intra-lesion vascularity, and a heterogeneous echotexture, were demonstrated in this case. They should prompt further investigation and onward referral.
Learning Point 3: While ultrasound is valuable for evaluating suspicious features of soft tissue lesions, gadolinium-enhanced MRI remains the gold standard for evaluating tumour extent and infiltrative spread. The tail sign of fascial spread was demonstrated in this case and is a key diagnostic sign, before formal histopathology confirmation (Figure 4-7).
6References
1. Lefkowitz RA, Landa J, Hwang S, Zabor EC, Moskowitz CS, Agaram NP, Panicek DM. Myxofibrosarcoma: prevalence and diagnostic value of the "tail sign" on magnetic resonance imaging. Skeletal Radiol. 2013 Jun;42(6):809-18. doi: 10.1007/s00256-012-1563-6. Epub 2013 Jan 15. PMID: 23318907; PMCID: PMC4082187.
2. https://www.bmus.org/mediacentre/news/new-soft-tissue-masses-guidelines/
2. https://www.bmus.org/mediacentre/news/new-soft-tissue-masses-guidelines/

{kind=link}