Rare Multinodular Epithelioid Malignant Mesothelioma of the Tunica Vaginalis [September 2025]
November 26, 2025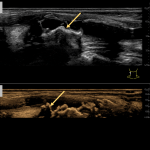
Vulnerable Plaque in Focus: A Multimodal Ultrasound Case Study with Triplex, High-Resolution Flow, and 3D Imaging [November 2025]
December 15, 2025
SUBMIT YOUR CASE
EFSUMB invites submission of interesting cases for the website section 'Case of the Month'. All CoM submissions are eligible for selection for free registration at the next Euroson congress. Two cases that receive the most 'likes' in a year will receive free registration for the next EUROSON congress and the third most liked liked case will receive a cash prize of 100 EUR.
The Double Aorta Artifact: A Benign Trap in Abdominal Sonography
Authors:
Pavlína Vyhnanovská [1], Dmitry Salomatin [2], Jan Kopecký [3]Affiliation:
[1] Third Faculty of Medicine, Department of Internal Medicine, Charles University and University Hospital Kralovske Vinohrady, Prague, Czechia[2] Third Faculty of Medicine, Department of Radiology and Nuclear Medicine, Charles University and University Hospital Kralovske Vinohrady, Prague, Czechia
[3] Canadian Medical Clinic, Prague 6 AFI, Prague, Czechia






1Clinical History
A 32-year-old man with an athletic build and no clinical problems comes for a preventive check-up.
2Image Findings
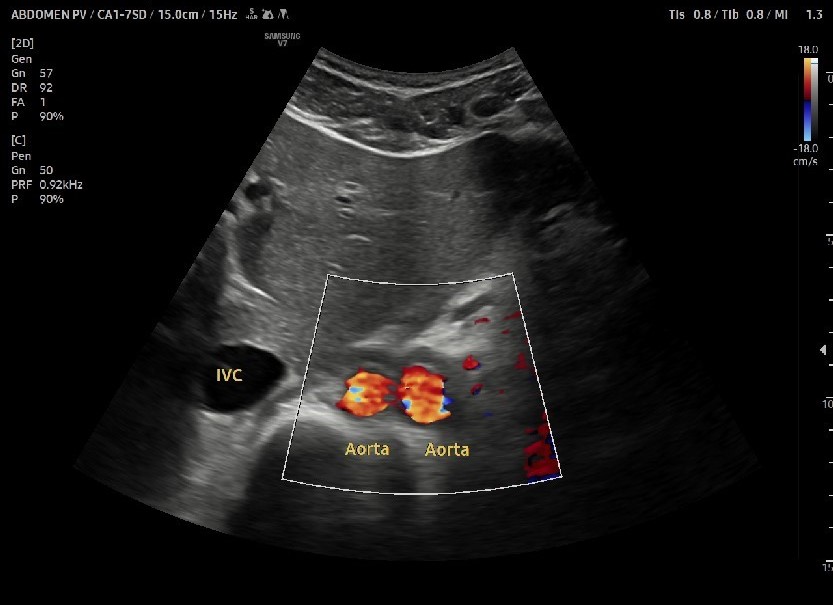
Fig. 1. Picture of the proximal abdominal aorta in the transverse plane using Doppler examination, showing two abdominal aorta lumina instead of a single lumen.
Fig. 2. Double Doppler artifact in a B-mode ultrasound image, which may simulate the presence of two vascular structures.
Fig. 3. Presents spectral Doppler recordings from a triplex ultrasound examination, illustrating flow patterns within both the right and left lumina of a double aorta artifact.
Fig. 4. An example of chronic dissection of the infrarenal abdominal aorta in the longitudinal plane in a 70-year-old patient. The dissection corresponds to a thin hyperechoic line in the aortic lumen.
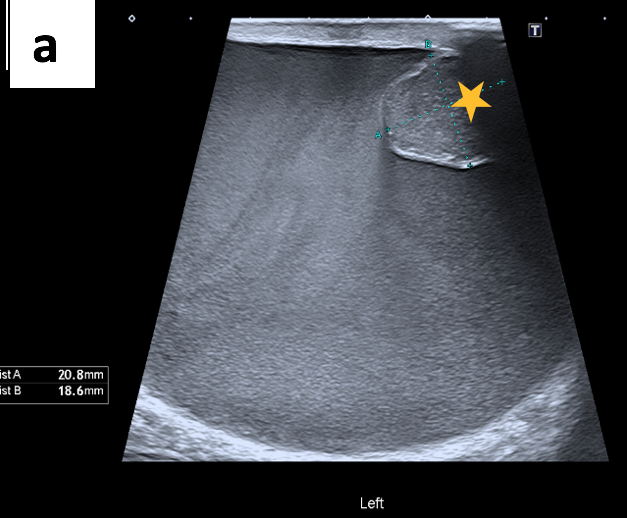
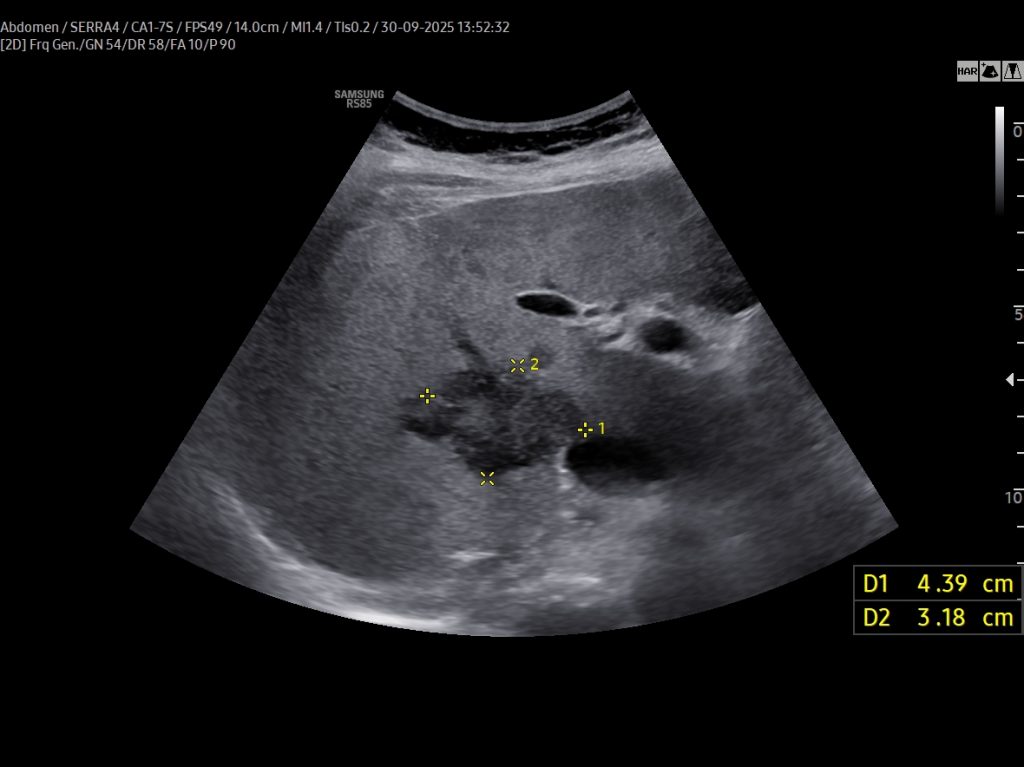
Fig. 5. 61-year-old patient with an infrarenal abdominal aortic aneurysm with a thrombotic rim intraluminal.
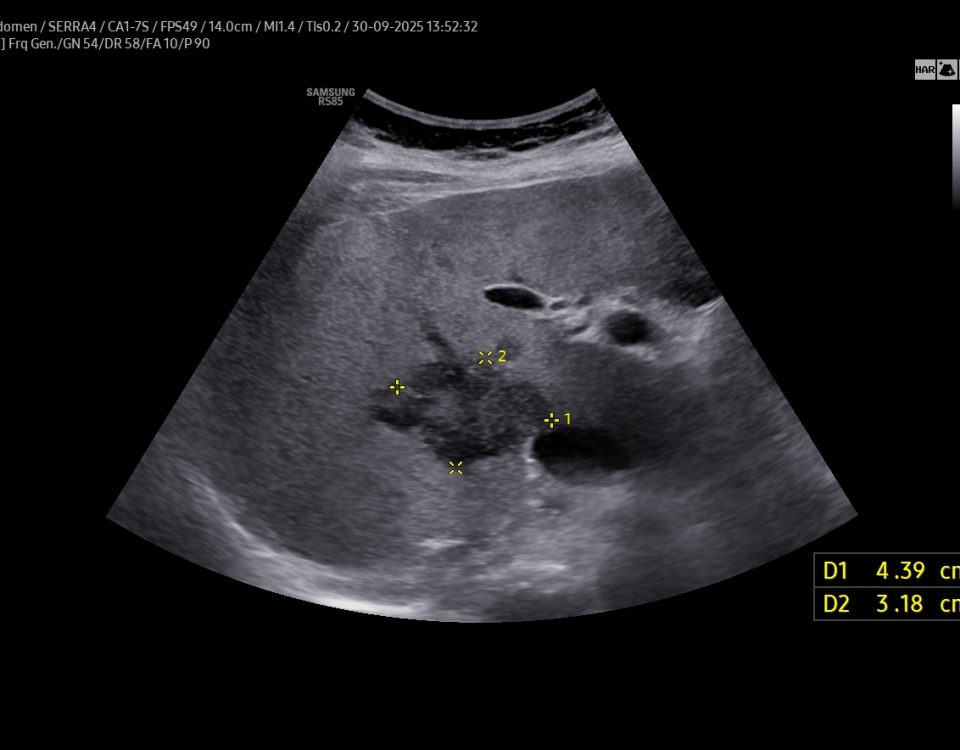
Fig. 6. A transverse ultrasound image of an 83-year-old female with a juxtarenal leaking abdominal aortic aneurysm accompanied by a retroperitoneal hematoma.
Fig. 7. Normal B-mode ultrasound image of the longitudinal abdominal aorta with no sign of the artifact. The linear hyperechoic structure (marked with a red arrow) corresponds to the ventral wall of the abdominal aorta.
Fig. 2. Double Doppler artifact in a B-mode ultrasound image, which may simulate the presence of two vascular structures.
Fig. 3. Presents spectral Doppler recordings from a triplex ultrasound examination, illustrating flow patterns within both the right and left lumina of a double aorta artifact.
Fig. 4. An example of chronic dissection of the infrarenal abdominal aorta in the longitudinal plane in a 70-year-old patient. The dissection corresponds to a thin hyperechoic line in the aortic lumen.
Fig. 5. 61-year-old patient with an infrarenal abdominal aortic aneurysm with a thrombotic rim intraluminal.
Fig. 6. A transverse ultrasound image of an 83-year-old female with a juxtarenal leaking abdominal aortic aneurysm accompanied by a retroperitoneal hematoma.
Fig. 7. Normal B-mode ultrasound image of the longitudinal abdominal aorta with no sign of the artifact. The linear hyperechoic structure (marked with a red arrow) corresponds to the ventral wall of the abdominal aorta.
3Diagnosis
Double aorta artifact
4Discussion
The double aorta artifact is a common sonographic phenomenon that appears as a duplicated abdominal aorta in transverse views, particularly on B-mode and colour Doppler imaging (see figures 1-3 of this patient).
Misinterpretation may lead to unnecessary concerns or invasive procedures. The phenomenon has been documented in medical literature since the 1970s–1990s and is an important consideration in abdominal ultrasound diagnostics to avoid false-positive diagnoses (1,2).
The described artifact arises from refractive distortion of the ultrasound beam at tissue interfaces with significant differences in echogenicity, such as between the fascia of the rectus abdominis muscles and adjacent structures, such as subcutaneous fat or liver tissue. Specifically, the interface acts like a prism, bending the ultrasound waves and producing the visual illusion of a duplicated vessel—most notably the abdominal aorta. How to Differentiate the Artifact from True Pathology? Alter the ultrasound beam angle so it does not cross the refractive interface, thereby reducing or eliminating the artifact. Rotating the transducer into a sagittal plane often diminishes the appearance of the double vessel.
Spectral Doppler (pulsed wave Doppler) waveforms remain physiologically normal in the presence of the artifact. They can be used to distinguish between actual pathology and artifact, as accurate duplications or dissections will show abnormal flow patterns.
The artifact is more common in younger individuals with well-developed abdominal musculature, which enhances tissue interfaces. The duplication seen is often partial rather than complete. Similar refractive artifacts may occur in other imaging modalities, such as transthoracic echocardiography, but less frequently. It is important to note that postprocessing in ultrasound systems enhances image quality and creates contrast transitions. When viewing the abdominal aorta longitudinally (Fig. 7), this can cause the ventral wall of the aorta to appear as a linear hyperechoic structure, which can be misinterpreted as an artifact (3).
Recognizing double aorta artifact is essential because it can mimic more serious conditions such as aortic dissection and abdominal aortic aneurysm (AAA) (Fig. 4-6)
Misinterpretation may lead to unnecessary concerns or invasive procedures. The phenomenon has been documented in medical literature since the 1970s–1990s and is an important consideration in abdominal ultrasound diagnostics to avoid false-positive diagnoses (1,2).
The described artifact arises from refractive distortion of the ultrasound beam at tissue interfaces with significant differences in echogenicity, such as between the fascia of the rectus abdominis muscles and adjacent structures, such as subcutaneous fat or liver tissue. Specifically, the interface acts like a prism, bending the ultrasound waves and producing the visual illusion of a duplicated vessel—most notably the abdominal aorta. How to Differentiate the Artifact from True Pathology? Alter the ultrasound beam angle so it does not cross the refractive interface, thereby reducing or eliminating the artifact. Rotating the transducer into a sagittal plane often diminishes the appearance of the double vessel.
Spectral Doppler (pulsed wave Doppler) waveforms remain physiologically normal in the presence of the artifact. They can be used to distinguish between actual pathology and artifact, as accurate duplications or dissections will show abnormal flow patterns.
The artifact is more common in younger individuals with well-developed abdominal musculature, which enhances tissue interfaces. The duplication seen is often partial rather than complete. Similar refractive artifacts may occur in other imaging modalities, such as transthoracic echocardiography, but less frequently. It is important to note that postprocessing in ultrasound systems enhances image quality and creates contrast transitions. When viewing the abdominal aorta longitudinally (Fig. 7), this can cause the ventral wall of the aorta to appear as a linear hyperechoic structure, which can be misinterpreted as an artifact (3).
Recognizing double aorta artifact is essential because it can mimic more serious conditions such as aortic dissection and abdominal aortic aneurysm (AAA) (Fig. 4-6)
5Teaching Points
1. Recognize the double aorta artifact to prevent misdiagnosis. Use adjustments in transducer positioning and angle to reduce the artifact. Confirm findings with spectral Doppler waveforms to differentiate actual pathology from artifacts.
2. Always consider clinical context and measurement criteria for AAA diagnosis. In cases of suspected aortic dissection or rupture, a comprehensive evaluation and correlation with clinical findings are recommended to confirm the diagnosis and avoid unnecessary interventions.
2. Always consider clinical context and measurement criteria for AAA diagnosis. In cases of suspected aortic dissection or rupture, a comprehensive evaluation and correlation with clinical findings are recommended to confirm the diagnosis and avoid unnecessary interventions.
6References
1. Hadzik R, Bombiński P, Brzewski M. Double aorta artifact in sonography - a diagnostic challenge. J Ultrason. 2017 Mar;17(68):36-40
2. Spieker LE, Hufschmid U, Oechslin E, Jenni R. Double aortic and pulmonary valves: An artifact generated by ultrasound refraction. J Am Soc Echocardiogr. 2004 Jul;17(7):786-7
3. Klee O, Buechler J, Fears M, Gosser C, Nix K. A Point of Care Ultrasound (POCUS) Artifact Mimicking an Aortic Dissection: A Case Series. POCUS J. 2025 Apr 15;10(1):88-91
2. Spieker LE, Hufschmid U, Oechslin E, Jenni R. Double aortic and pulmonary valves: An artifact generated by ultrasound refraction. J Am Soc Echocardiogr. 2004 Jul;17(7):786-7
3. Klee O, Buechler J, Fears M, Gosser C, Nix K. A Point of Care Ultrasound (POCUS) Artifact Mimicking an Aortic Dissection: A Case Series. POCUS J. 2025 Apr 15;10(1):88-91
{kind=link}