The eyes cannot see what the mind does not know. Ultrasound-based diagnosis of aorto-mesenteric clamp syndrome in the emergency department [February 2024]
July 3, 2024
Midgut malrotation and volvulus with bowel necrosis after HPS operation [April 2024]
July 18, 2024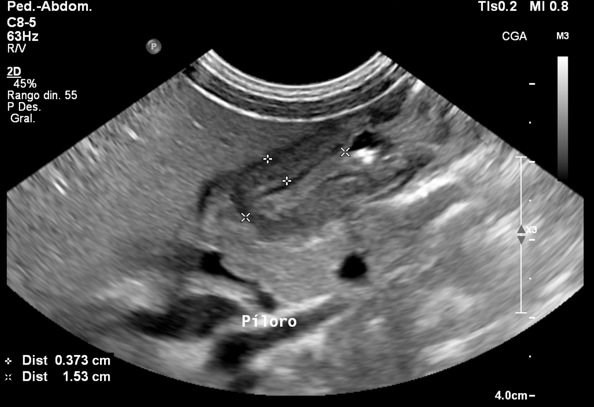
SUBMIT YOUR CASE
EFSUMB invites submission of interesting cases for the website section 'Case of the Month'. All CoM submissions are eligible for selection for free registration at the next Euroson congress. Two cases that receive the most 'likes' in a year will receive free registration for the next EUROSON congress and the third most liked liked case will receive a cash prize of 100 EUR.
Breaking the Barrier: Ultrasound Diagnosis of Infantile Hypertrophic Pyloric Stenosis
Authors: Md. Michelle Narvaez, Md. Carolina Saenz, Dra. Lucia Gomez
The Radiology Department of Metropolitan Hospital, Quito, Ecuador.
International University of Ecuador.

1Clinical History
A 2-month-old male patient presents with projectile postprandial nonbilious vomiting of 24 hours duration, associated with irritability and excessive sialorrhea. On physical examination, the abdomen is tender to both superficial and deep palpation in the epigastric region. Laboratory tests show all parameters within normal limits.
2 Abdominal Ultrasound Findings
The pylorus is enlarged (Fig.1,2):
• Muscle Wall Thickness: 4.6 mm
• Pyloric Channel Length: 16 mm
• Transverse Diameter: 11 mm
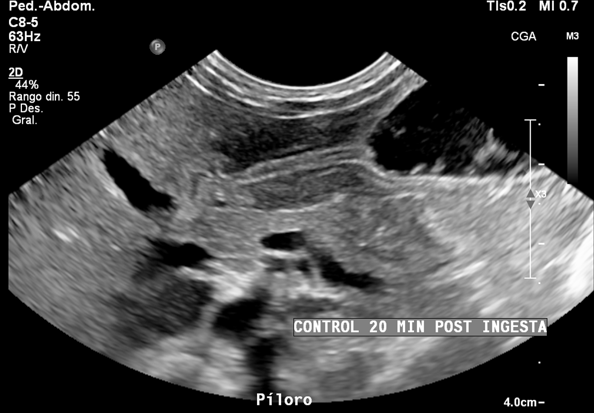
During the ultrasound examination, the patient was fed maternal milk. After 20 minutes, the stomach remained filled with the ingested milk, showing waves of tachygastria without passage through the pylorus into the duodenum (Fig.3).
Based on the clinical symptoms and abdominal ultrasound imaging, the clinical diagnosis was hypertrophic pyloric stenosis. Surgical intervention is considered to be a curative treatment.
• Muscle Wall Thickness: 4.6 mm
• Pyloric Channel Length: 16 mm
• Transverse Diameter: 11 mm
During the ultrasound examination, the patient was fed maternal milk. After 20 minutes, the stomach remained filled with the ingested milk, showing waves of tachygastria without passage through the pylorus into the duodenum (Fig.3).
Based on the clinical symptoms and abdominal ultrasound imaging, the clinical diagnosis was hypertrophic pyloric stenosis. Surgical intervention is considered to be a curative treatment.
3Diagnosis
Infantile Hypertrophic Pyloric Stenosis
4Discussion
Infantile hypertrophic pyloric stenosis (IHPS) is a common condition in infants, typically presenting between 2 to 8 weeks of age, characterized by the hypertrophy of the pyloric muscle, leading to gastric outlet obstruction.
IHPS affects approximately 2-4 per 1,000 live births, with a higher incidence in male infants. The condition commonly presents with projectile vomiting, which is often non-bilious, and may be associated with symptoms such as irritability, excessive hunger, and dehydration. Physical examination may reveal a palpable "olive" mass in the epigastric region, and infants often exhibit signs of malnutrition and weight loss due to vomiting.
Ultrasound is the preferred diagnostic modality for IHPS due to its high sensitivity and specificity, non-invasiveness, and absence of radiation exposure.
High-frequency transducers are essential for examining IHPS. A linear transducer operating between 6 and 10 MHz, adjusted to the infant's size and pylorus depth, is typically used.
The characteristic ultrasound findings include:
- Muscle Wall Thickness: typically, greater than 3 mm.
- Pyloric Channel Length: greater than 15-18 mm.
- Transverse Diameter: increased, often more than 11 mm
The treatment of IHPS has evolved significantly, marked by key surgical innovations and a remarkable decline in patient mortality. Early nonsurgical treatments included nutrient enemas and gastric lavage, while pharmacologic agents such as atropine and belladonna were also used. The first surgical intervention began in 1892, with gastroenterostomy, followed by pyloroplasty in the early 20th century. The Ramstedt procedure, first performed in 1911, became the standard surgical treatment, reducing mortality rates to below 2% today, reflecting a significant medical success.
The ultrasound examination of the pylorus is a dynamic process that requires a systematic approach. Radiologists need to be aware of potential challenges and know strategies to address them. Familiarity with both normal and hypertrophied pyloric appearances is crucial, as it enhances diagnostic accuracy and aids in the early diagnosis and effective management of infants with hypertrophic pyloric stenosis
IHPS affects approximately 2-4 per 1,000 live births, with a higher incidence in male infants. The condition commonly presents with projectile vomiting, which is often non-bilious, and may be associated with symptoms such as irritability, excessive hunger, and dehydration. Physical examination may reveal a palpable "olive" mass in the epigastric region, and infants often exhibit signs of malnutrition and weight loss due to vomiting.
Ultrasound is the preferred diagnostic modality for IHPS due to its high sensitivity and specificity, non-invasiveness, and absence of radiation exposure.
High-frequency transducers are essential for examining IHPS. A linear transducer operating between 6 and 10 MHz, adjusted to the infant's size and pylorus depth, is typically used.
The characteristic ultrasound findings include:
- Muscle Wall Thickness: typically, greater than 3 mm.
- Pyloric Channel Length: greater than 15-18 mm.
- Transverse Diameter: increased, often more than 11 mm
The treatment of IHPS has evolved significantly, marked by key surgical innovations and a remarkable decline in patient mortality. Early nonsurgical treatments included nutrient enemas and gastric lavage, while pharmacologic agents such as atropine and belladonna were also used. The first surgical intervention began in 1892, with gastroenterostomy, followed by pyloroplasty in the early 20th century. The Ramstedt procedure, first performed in 1911, became the standard surgical treatment, reducing mortality rates to below 2% today, reflecting a significant medical success.
The ultrasound examination of the pylorus is a dynamic process that requires a systematic approach. Radiologists need to be aware of potential challenges and know strategies to address them. Familiarity with both normal and hypertrophied pyloric appearances is crucial, as it enhances diagnostic accuracy and aids in the early diagnosis and effective management of infants with hypertrophic pyloric stenosis
5Teaching Points
• Hypertrophic Pyloric Stenosis is characterized by thickening of the muscle layer and a lack of relaxation in the pyloric canal.
• The primary diagnostic criterion is a measurement of the muscular layer thickness exceeding 3mm.
• Abnormal elongation of the canal is defined as a length greater than 12 mm.
• The primary diagnostic criterion is a measurement of the muscular layer thickness exceeding 3mm.
• Abnormal elongation of the canal is defined as a length greater than 12 mm.
6Keywords
Infantile hypertrophic pyloric stenosis, Ultrasound.
7References
1. Hernanz-Schulman M. Infantile hypertrophic pyloric stenosis. Radiology. 2003;227:319–331.
2. Hiorns MP. Gastrointestinal tract imaging in children: current techniques. Pediatr Radiol. 2011;41:42–54.
3. Reed AA, Michael K. Hypertrophic pyloric stenosis. J Diagn Med Sonography. 2010;26:157–160.
4. Haider N, Spicer R, Grie D (2002) Ultrasound diagnosis of infantile hypertrophic pyloric stenosis: determinants of pyloric length and the effect of prematurity. Clin Radiol 57:136–139
5. Nasr A, Ein SH, Connolly B. Recurrent pyloric stenosis: to dilate or operate? A preliminary report. J Pediatr Surg. 2008;43:E17–E20.
6. Yoshizawa J, Eto T, Higashimoto Y, Saitou T, Maie M. Ultrasonographic features of normalization of the pylorus after pyloromyotomy for hypertrophic pyloric stenosis. J Pediatr Surg. 2001;36:582–586.
7. Rohrschneider WK, Mittnacht H, Darge K, Tröger J. Pyloric muscle in asymptomatic infants: sonographic evaluation and discrimination from idiopathic hypertrophic pyloric stenosis. Pediatr Radiol. 1998;28:429–434.
8. González Hernández G, Ferreira Moreno V. Estenosis hipertrófica del píloro. Diagnóstico por imágenes. Rev Méd Electrón [Internet]. 2007 [citado 24 Jun 2024];29(2).
9. Panteli C. New insights into the pathogenesis of infantile pyloric stenosis. Pediatr Surg Int. 2009;25:1043–1052.
10. Chandran L, Chitkara M. Vomiting in children: reassurance, red flag, or referral? Pediatr Rev. 2008;29:183–192.
2. Hiorns MP. Gastrointestinal tract imaging in children: current techniques. Pediatr Radiol. 2011;41:42–54.
3. Reed AA, Michael K. Hypertrophic pyloric stenosis. J Diagn Med Sonography. 2010;26:157–160.
4. Haider N, Spicer R, Grie D (2002) Ultrasound diagnosis of infantile hypertrophic pyloric stenosis: determinants of pyloric length and the effect of prematurity. Clin Radiol 57:136–139
5. Nasr A, Ein SH, Connolly B. Recurrent pyloric stenosis: to dilate or operate? A preliminary report. J Pediatr Surg. 2008;43:E17–E20.
6. Yoshizawa J, Eto T, Higashimoto Y, Saitou T, Maie M. Ultrasonographic features of normalization of the pylorus after pyloromyotomy for hypertrophic pyloric stenosis. J Pediatr Surg. 2001;36:582–586.
7. Rohrschneider WK, Mittnacht H, Darge K, Tröger J. Pyloric muscle in asymptomatic infants: sonographic evaluation and discrimination from idiopathic hypertrophic pyloric stenosis. Pediatr Radiol. 1998;28:429–434.
8. González Hernández G, Ferreira Moreno V. Estenosis hipertrófica del píloro. Diagnóstico por imágenes. Rev Méd Electrón [Internet]. 2007 [citado 24 Jun 2024];29(2).
9. Panteli C. New insights into the pathogenesis of infantile pyloric stenosis. Pediatr Surg Int. 2009;25:1043–1052.
10. Chandran L, Chitkara M. Vomiting in children: reassurance, red flag, or referral? Pediatr Rev. 2008;29:183–192.

{kind=link}