
Anaplastic giant cell lymphoma (ALCG) associated with breast implants [APRIL 2025]
July 23, 2025
CO-CHAIR – Dirk Clevert
August 27, 2025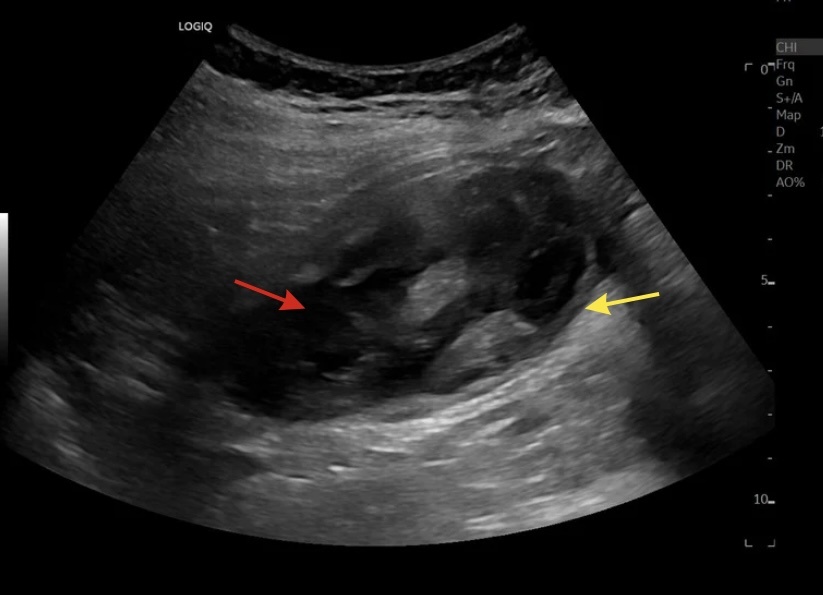
SUBMIT YOUR CASE
EFSUMB invites submission of interesting cases for the website section 'Case of the Month'. All CoM submissions are eligible for selection for free registration at the next Euroson congress. Two cases that receive the most 'likes' in a year will receive free registration for the next EUROSON congress and the third most liked liked case will receive a cash prize of 100 EUR.
An unexpected guest beneath the liver
Authors:
Jovana Tumanov1, Dragan Vasin1, Nikola Grubor2,Jelena Čavić3,Tijana Tomić1
1. Emergency Radiology Department, 2. Institute for Medical Statistics and Informatics, 3. Institute of Pathology, University Clinical Centre of Serbia, 11000 Belgrade, Republic of Serbia,

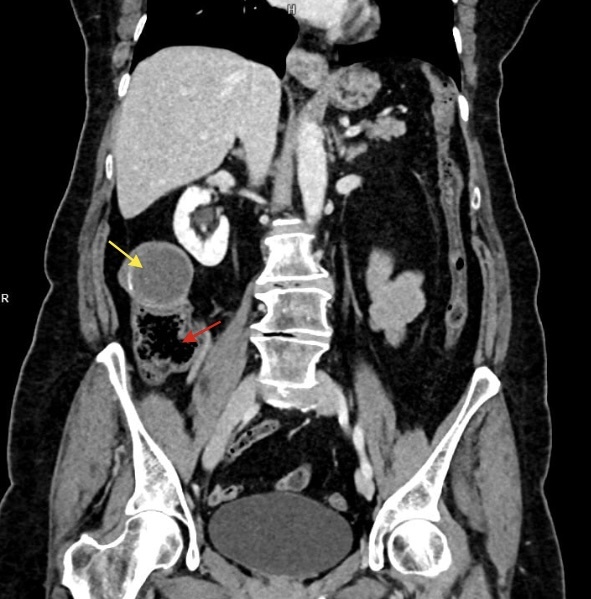
Figure 3. Coronal plane: The yellow arrow indicates the lumen of the lesion measuring up to 100 x 60 x 90 mm (AP x transverse x craniocaudal with the craniocaudal diameter measured in the sagittal plane) contains material of density up to 20HU in the non-contrast phase. The red arrow show the caecum from which the lesion appers to arise. No lymphadenopathy is seen.
1Clinical History
The female patient reports experiencing intermittent pain in the right upper quadrant over the past few months initially described as stabbing in nature. The pain has recently become more of a dull, pressure-like discomfort without radiation. On physical examination, there is tenderness to both superficial and deep palpation in the mid-right abdominal region. The liver was not palpable as enlarged.
Inflammatory markers are within normal limits, while a mildly elevated tumor marker CEA has been observed.
The patient has a history of total hysterectomy with bilateral adnexectomy performed ten years ago - Histopathologically confirmed diagnosis of microinvasive squamous cell carcinoma of the uterine cervix.
Inflammatory markers are within normal limits, while a mildly elevated tumor marker CEA has been observed.
The patient has a history of total hysterectomy with bilateral adnexectomy performed ten years ago - Histopathologically confirmed diagnosis of microinvasive squamous cell carcinoma of the uterine cervix.
2Image Findings
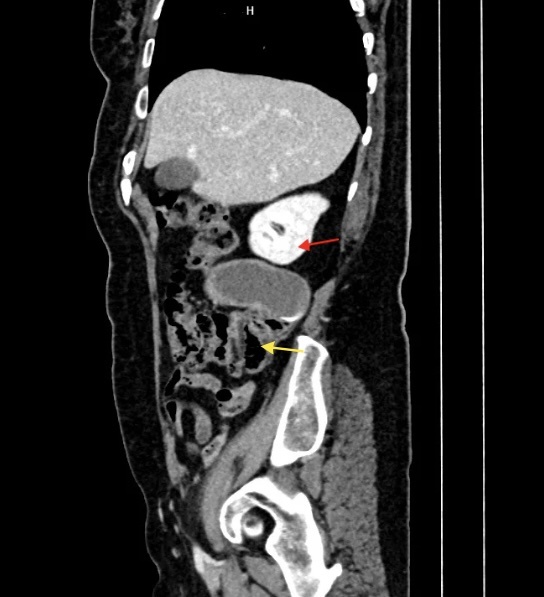
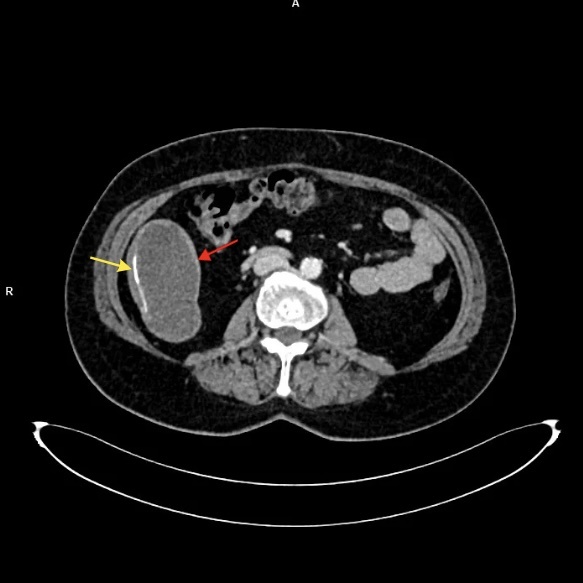
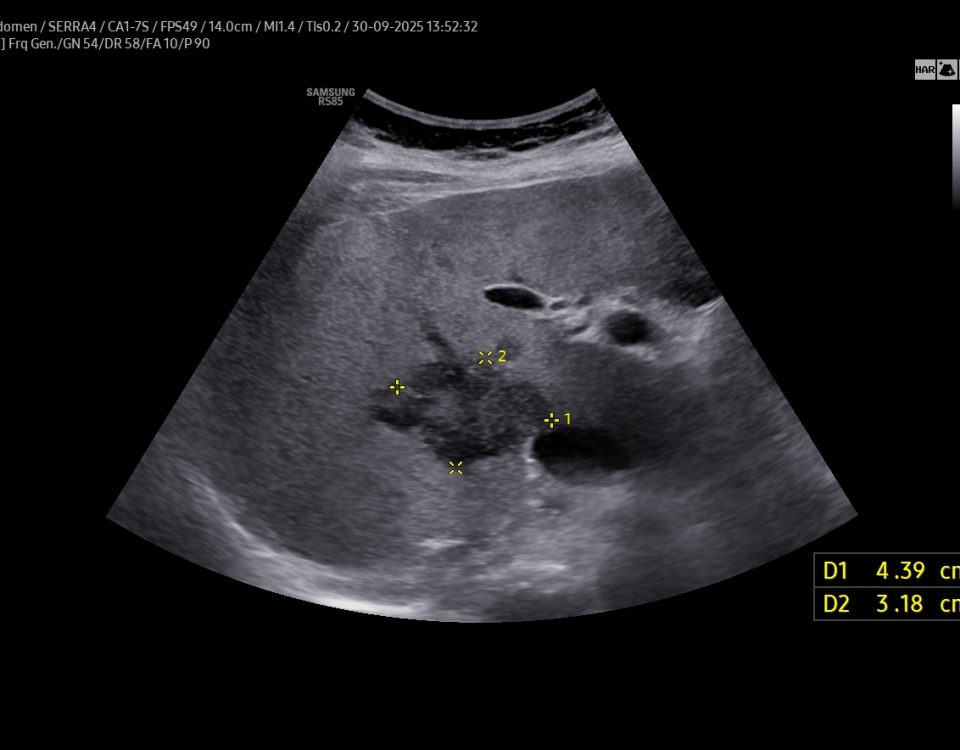
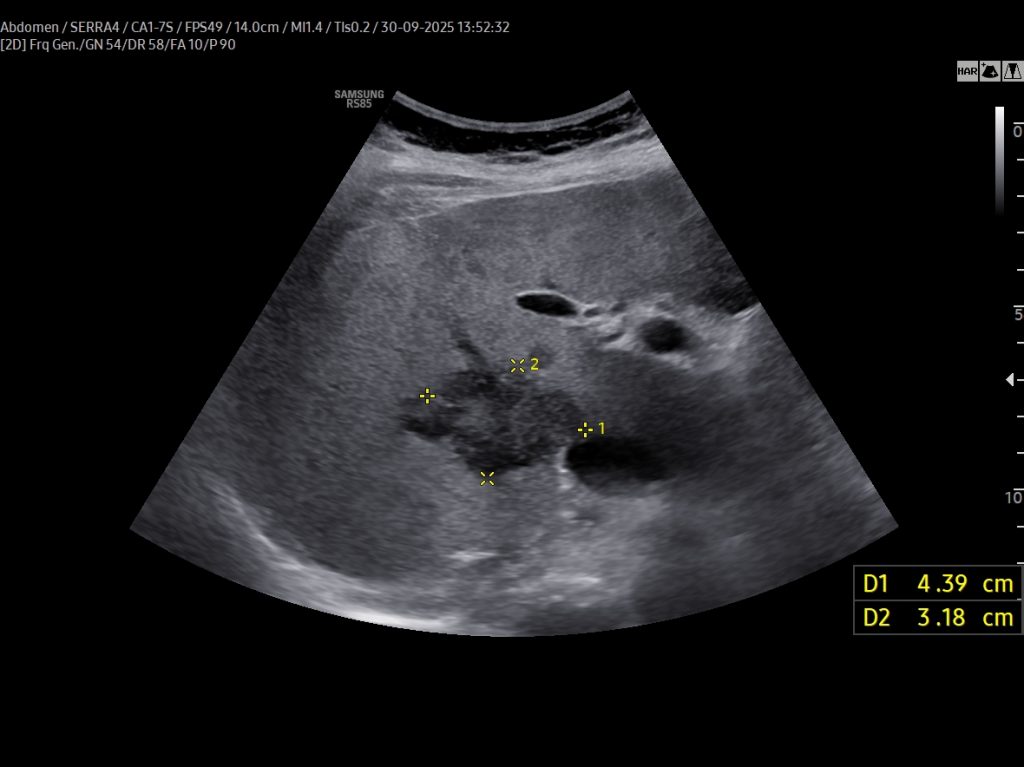
At ultrasonography (US) a large cystic lesion (up to 10 cm) was seen in the right upper and middle quadrant without internal vascular flow on color Doppler imaging (Fig.1,2, Movie 1). This is not a typical location for the appendix which it is usually found lower in the abdomen. CT scan confirmed the presence of the lesion (100 x 60 x 90 mm in size ) arising from the caecum and containing dense material in the lumen (Fig.3,4). The lesion had clearly delineated , well-formed wall, partially calcified (Fig.5). No lymphadenopathy was seen.
3Differential Diagnosis
There were differential diagnostic dilemmas regarding the origin of the lesion (e.g., mesenteric cyst, right adnexal cyst, retroperitoneal lesion...). There was medial displacement of the ascending colon loop, indicating that the mass was not only large but also mechanically significant, potentially causing clinical symptoms such as obstruction, pain, or altered peristalsis. Apparently, there were no signs of acute clinical presentation, nor the typical pain in the lower right quadrant. CT scan established the final diagnosis as possible appendiceal mucocele.
4Discussion
Atypical features in our case of appendiceal mucocele include its unusual position, the presence of a mass effect on surrounding structures, and the exclusion of suspicion for appendicitis. Appendiceal mucocele can rarely present with ileocolic intussusceptions. Radiologists, pathologists, primary care physicians and surgeons must be aware of this condition.
THERAPEUTIC APPROACH:
The definitive treatment for appendiceal mucocele is surgical removal, typically by appendectomy. The surgical approach depends on the size, location, and presence of complications. Simple mucocele without suspicion of malignancy is usually treated with laparoscopic or open appendectomy.
OUTCOME & PROGNOSIS:
Accurate preoperative diagnosis and early surgical treatment of appendiceal mucocele is important to prevent complications like pseudomyxoma peritonei, which has poor prognosis.
THERAPEUTIC APPROACH:
The definitive treatment for appendiceal mucocele is surgical removal, typically by appendectomy. The surgical approach depends on the size, location, and presence of complications. Simple mucocele without suspicion of malignancy is usually treated with laparoscopic or open appendectomy.
OUTCOME & PROGNOSIS:
Accurate preoperative diagnosis and early surgical treatment of appendiceal mucocele is important to prevent complications like pseudomyxoma peritonei, which has poor prognosis.
5Teaching Points
1. Appendiceal mucocele should be considered in patients with a well-defined, cystic, tubular structure in the right lower quadrant on ultrasound, especially when the lesion appears anechoic or contains internal echoes without vascular flow.
2. Differential Diagnosis:Key considerations for a cystic lesion in the right lower quadrant include mesenteric cyst, right adnexal cyst, and retroperitoneal lesions such as lymphangioma or pseudocyst. Precise assessment of lesion location, relation to adjacent structures, and internal features on ultrasound and CT is crucial to distinguish appendiceal mucocele from these entities.
3: Early recognition of appendiceal mucocele is crucial, as rupture may lead to pseudomyxoma peritonei—a potentially life-threatening complication requiring complex surgical management.
2. Differential Diagnosis:Key considerations for a cystic lesion in the right lower quadrant include mesenteric cyst, right adnexal cyst, and retroperitoneal lesions such as lymphangioma or pseudocyst. Precise assessment of lesion location, relation to adjacent structures, and internal features on ultrasound and CT is crucial to distinguish appendiceal mucocele from these entities.
3: Early recognition of appendiceal mucocele is crucial, as rupture may lead to pseudomyxoma peritonei—a potentially life-threatening complication requiring complex surgical management.
6References
1. Caracappa D, Gullà N, Gentile D, et al. Appendiceal mucocele. A case report and literature review. Ann Ital Chir. 2011; 82(3): 239-45.
2. Bejiga G. Appendiceal mucocele presenting as a leading point in ileocolic intussusceptions: "Case report". Int J Surg Case Rep. 2022; 96: 107307.
3. Mouden MAAE, Laalim SA. A huge appendiceal mucocele. Pan Afr Med J. 2022; 43: 123.
2. Bejiga G. Appendiceal mucocele presenting as a leading point in ileocolic intussusceptions: "Case report". Int J Surg Case Rep. 2022; 96: 107307.
3. Mouden MAAE, Laalim SA. A huge appendiceal mucocele. Pan Afr Med J. 2022; 43: 123.
{kind=link}