CEUS LI RADS
January 19, 2017
(Ch:38) 50th Anniversary Booklet
March 6, 2017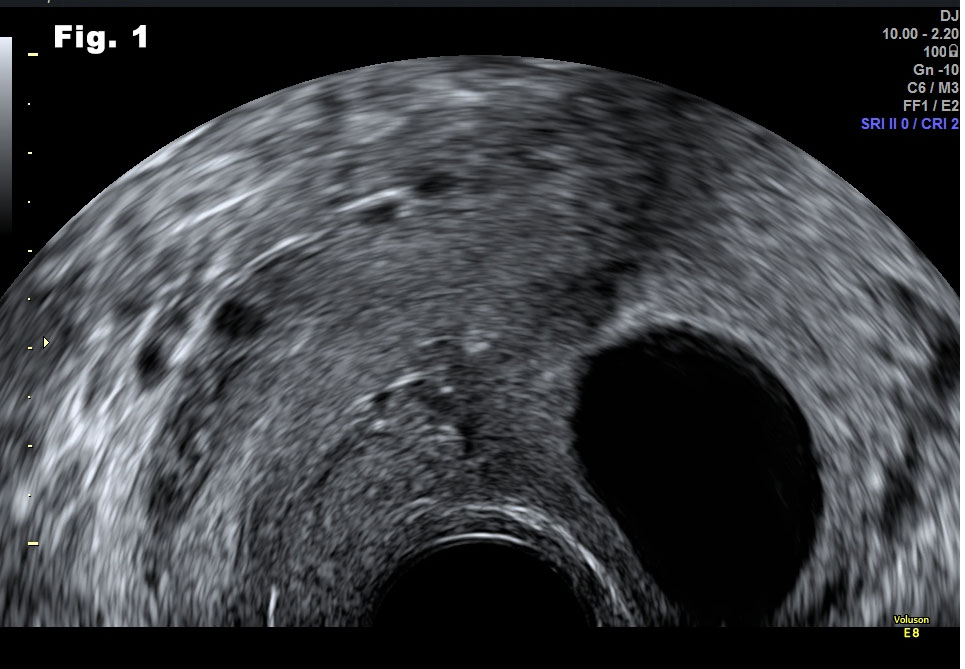
Cystic fibroids: A 40 years old, Caucasian, G2P2, visited the outpatient clinic of a tertiary university hospital with the complaint that on routine U/S scan multilocular cysts were detected.
Clinical Research Fellow, 3rd Dept of Obstetrics and Gynecology, Attikon General Hospital
University of Athens, Greece.
1 Rimini str, Chaidari, Athens PC 12462
TEL: 00302105832244
Corresponding Author:
Dr Grigorios Derdelis MD, MSc
Obstetrician-Gynecologist
grigorios.derdelis@yahoo.com
![Cystic fibroids</br> [Feb 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotm-feb2017-fig1.jpg)
![Cystic fibroids</br> [Feb 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotm-feb2017-fig2.jpg)
![Cystic fibroids</br> [Feb 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotm-feb2017-fig3.jpg)
![Cystic fibroids</br> [Feb 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotm-feb2017-fig4.jpg)
A 40 years old, Caucasian, G2P2, visited the outpatient clinic of a tertiary university hospital with the complaint that on routine U/S scan multilocular cysts were detected. These cysts were considered as suspicious of ovarian cancer, by a private gynecologist.
She was on oral Progesterone during the last years because of irregular vaginal bleeding. Last smear was normal 2 years before presenting to our clinic.
On transvaginal scan, an enlarged multilocular cyst was noted. The cyst was confined to the uterus and the endometrial cavity could be clearly seen on its entire length (fig. 1). The endometrium was thin as the patient was still under the influence of Progesterone.
The uterine multilocular cyst was avascular on Doppler examination and maximal diameter was 8cm (fig.2). The septations were thick and fibrotic, as well as avascular. The fluid was anechoic and there were no papillary projections.
Both ovaries were morphologically normal. All pelvic organs were mobile and the patient did not complain about pain during the examination. Trans-abdominal scan confirmed the diagnosis of the transvaginal scan (fig 3, 4). All these regular, rounded and avascular masses detected on ultrasound were suggestive of benign lesions. We offered to the patient a transvaginal needle biopsy to confirm the diagnosis. Cytology of aspirated fluid was negative for malignancy and a follow up scan in six months' time was recommended.
Uterine fibroids are common in women of Mediterranean, Caribbean and African origin. Nearly 40% of the peri-menopausal women have fibroids. In some women, for unknown reasons, fibroids undergo necrosis. Progesterone may play a role in those who have specific receptors on the fibroids. Cystic changes in fibroids are the result of necrosis that usually present with pain, although sometimes, they can be free of symptoms. Cystic fibroids may be confused with ovarian malignancy1,2 , retroperitoneal masses3 or even broad ligament masses4. On ultrasound examination, it is of paramount importance to detect the origin of the lesion. A uterine lesion has different prognosis from an ovarian or any other adnexal lesion. The endometrial cavity should be clearly seen on all its length and in continuity with the endocervix. A diagnostic challenge could be a pedunculated fibroid, but then the vascular stalk can be visualized, even during necrosis. Doppler examination is also crucial to visualize peripheral vasculature and exclude ''abnormal'' circulation pattern. Benign findings can be monitored over time and management can be tailored to the patient needs before been unnecessarily rushed to the operating theatre.
Ann Acad Med Singapore. 2004 May;33(3):371-4.
2
. Hacivelioglu S, Erkanli S. A large pedunculated leiomyoma with two-sided cystic degenerations mimicking a bilateral ovarian malignancy: a case report.
Eur J Gynaecol Oncol. 2014;35(2):192-4.
3. Naykı Ü, Naykı C, Uluğ P, Yılmaz I, Cetin Z, Yıldırım Y. A rare case of a giant cystic leiomyoma presenting as a retroperitoneal mass.
Iran J Reprod Med. 2014 Dec;12(12):831-4.
4. Naz Masood S, Masood Y, Mathrani J.Diagnostic dilemma in Broad Ligament Leiomyoma with Cystic Degeneration.
Pak J Med Sci. 2014 Mar;30(2):452-4.
Figure 2: Transvaginal scan ,transverse view. Lesion-measuring 80mm. Normal myometrium (white arrow) on the right.
Figure 3:Trans-abdominal scan, longitudinal view. Dimensions of the multilocular lesion, measuring 80x80mm.
Figure 4: Trans-abdominal scan, transverse view. Lesion and normal myometrium (white arrow) on the right.

{kind=link}