Midgut malrotation and volvulus with bowel necrosis after HPS operation [April 2024]
July 18, 2024
Primary or metastatic tumor? – A case report of mucinous adenocarcinoma of pancreas [JUNE 2024]
July 29, 2024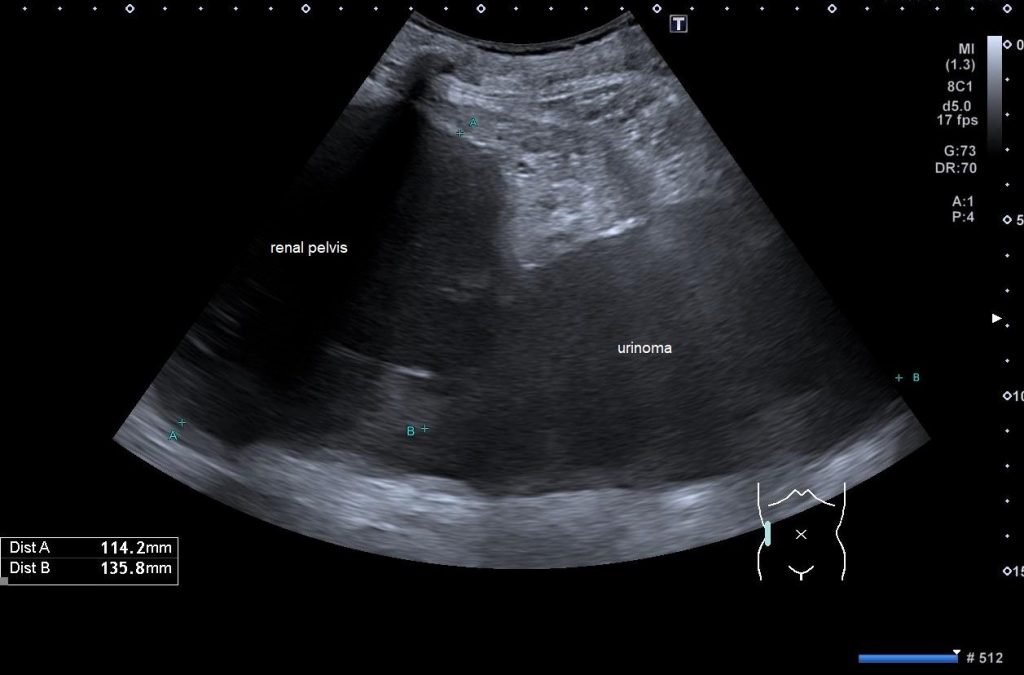
SUBMIT YOUR CASE
EFSUMB invites submission of interesting cases for the website section 'Case of the Month'. All CoM submissions are eligible for selection for free registration at the next Euroson congress. Two cases that receive the most 'likes' in a year will receive free registration for the next EUROSON congress and the third most liked liked case will receive a cash prize of 100 EUR.
Spontaneous Rupture of the Renal Pelvis with Large Urinoma
Authors: Pavlína Vyhnanovská [1], Václav Janík [2], Martin Michna [2]
[1]Department of Medicine, University Hospital Královské Vinohrady, Prague, Czech Republic
[2]Department of Radiology, University Hospital Královské Vinohrady, Prague, Czech Republic
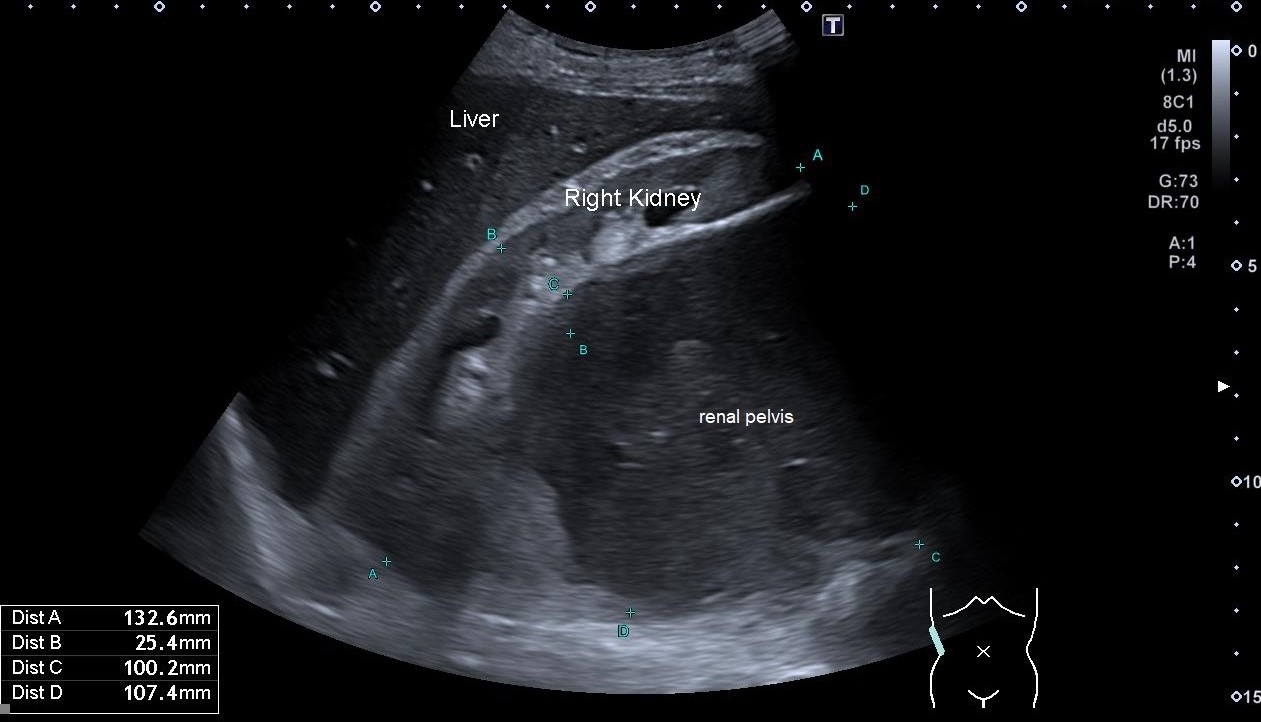
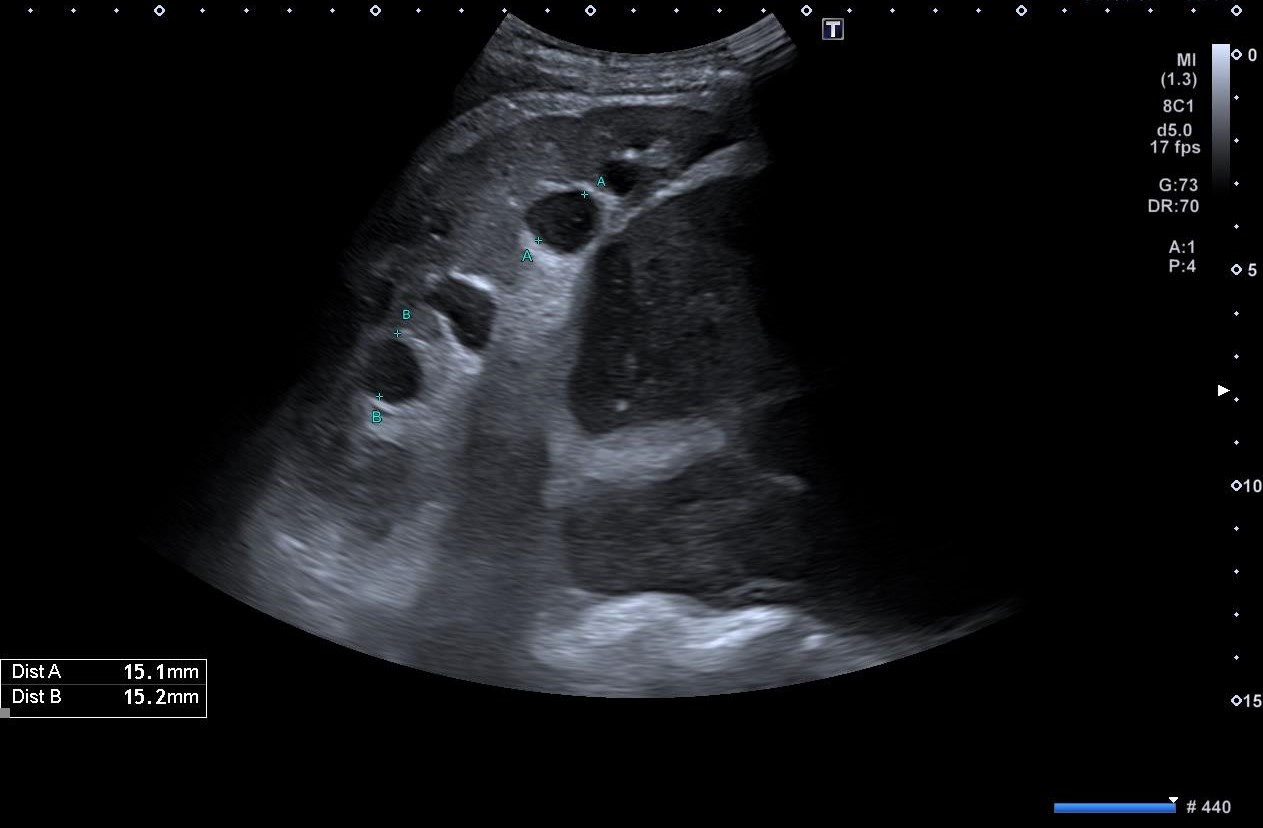
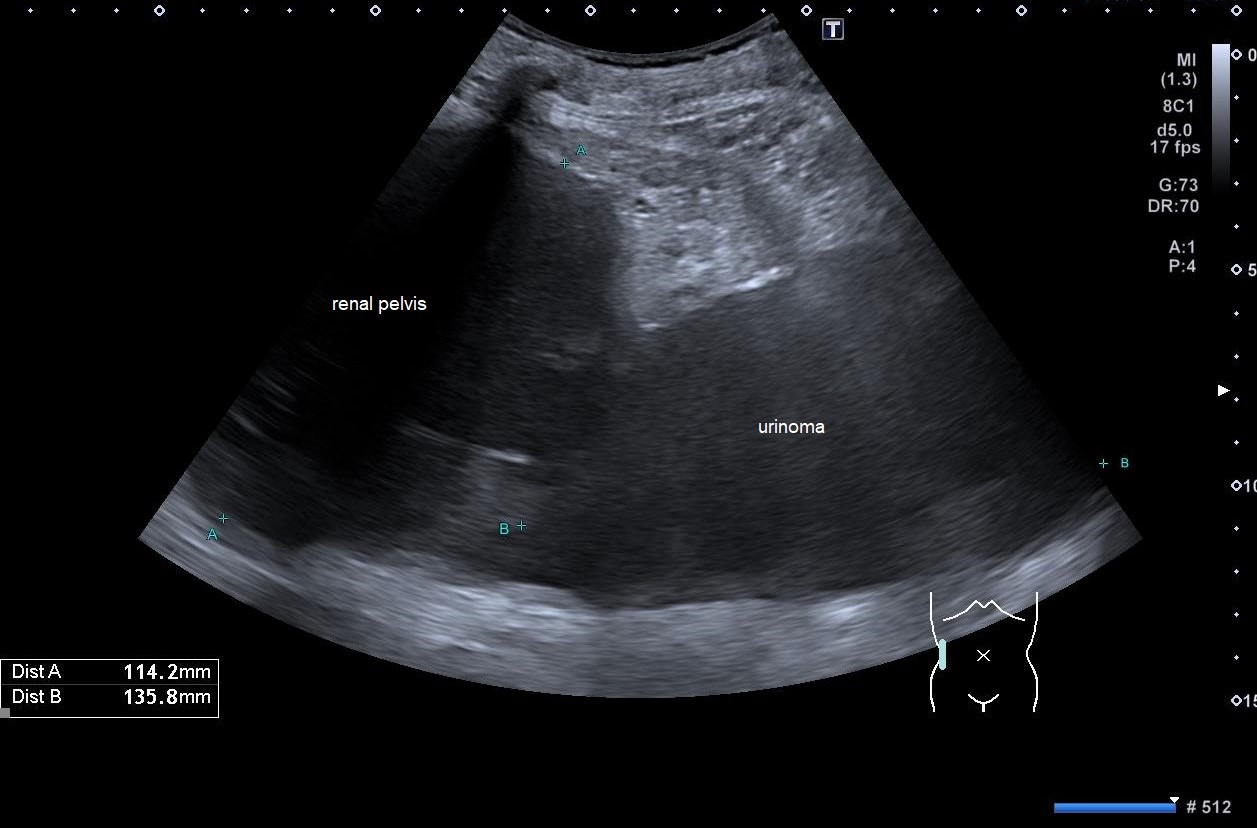
Figure 4. The video shows the continuity between the calyces and the cystic lesion corresponding to the pelvis.
1Clinical History
A 55-year-old man of low socio-economic status was admitted to the Internal Medicine department for sepsis and malnutrition. Four months prior to admission, he was treated for an abscess of the right iliac muscle which resulted in sepsis. Surgical drainage of a liquefied hematoma was performed.
2Image Findings
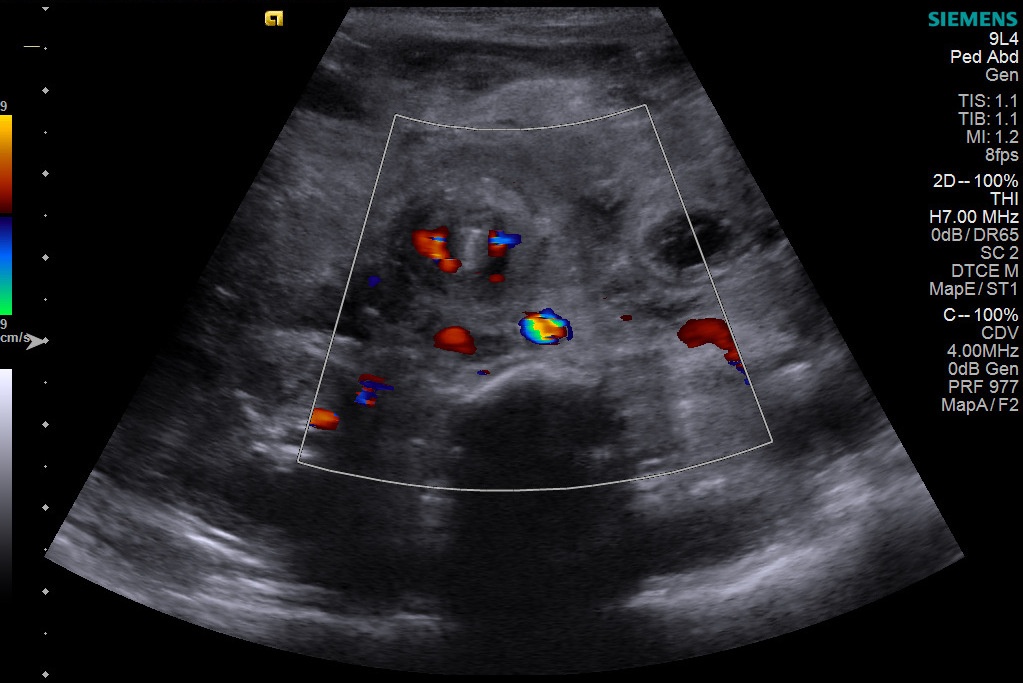
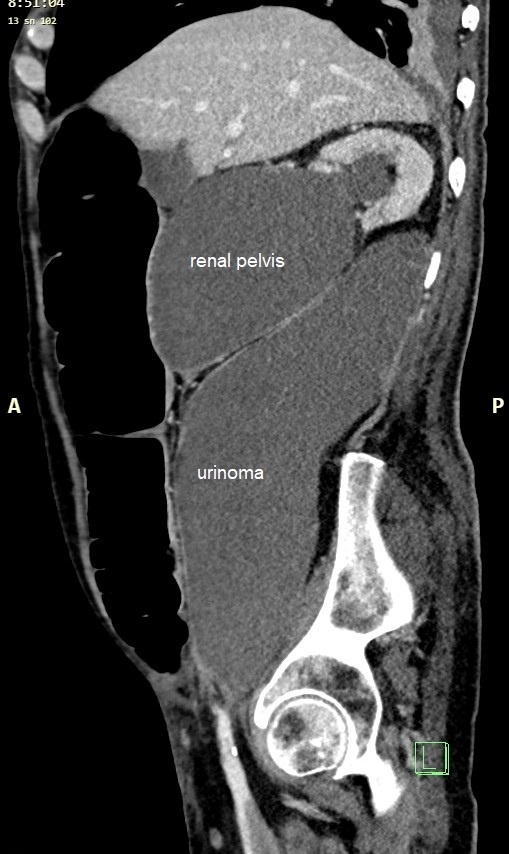
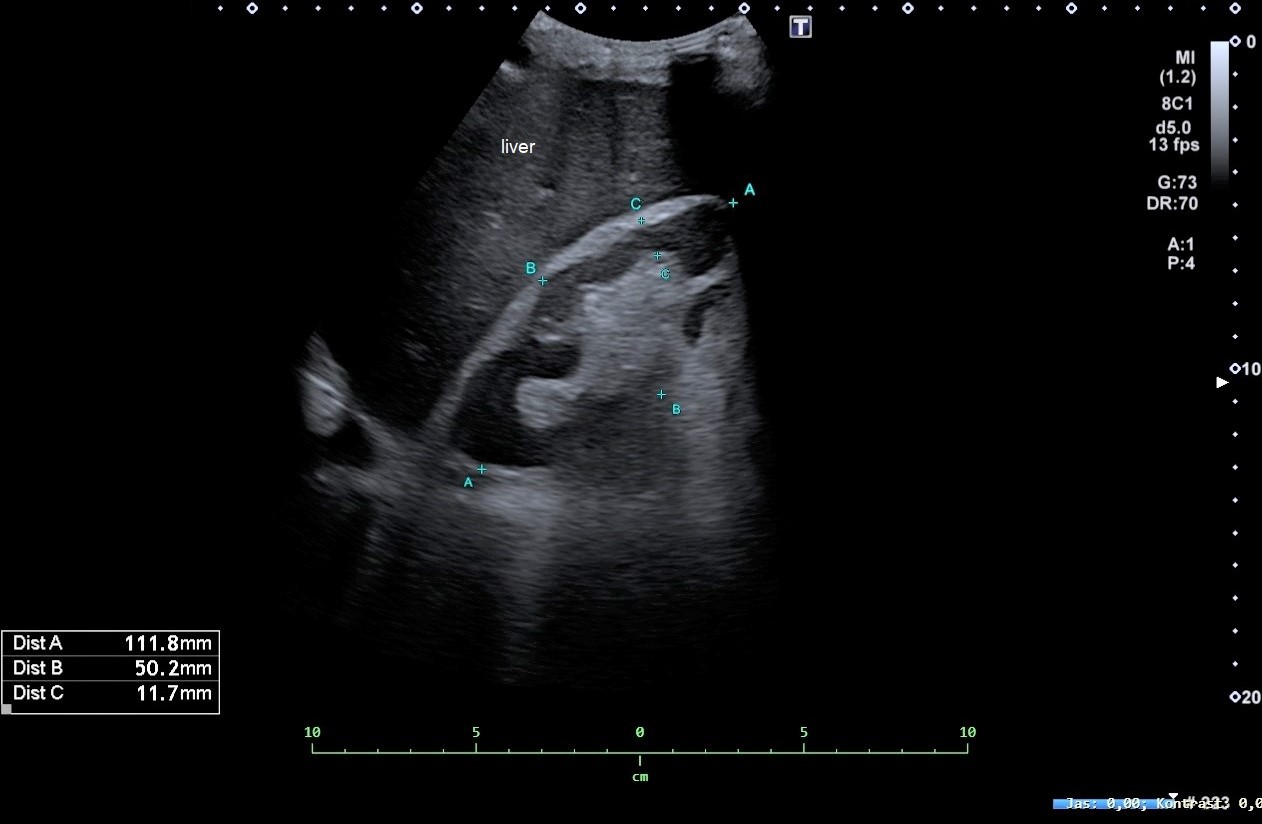
On abdominal ultrasound examination, two large cystic inhomogeneous fluid collections were found in the right mesogastrium. The more cranially located lesion was in close relationship with the kidney causing compression of urinary tract. The renal calyces were dilated, and their content was inhomogeneous (Figures 1-3). The close relationship of the more cranially located lesion to the kidney is evident in the video recording (Figure 4). Computed tomography scan (CT) with IV contrast showed a rupture of the right kidney and a large collection of fluid corresponding to a urinoma caudal to the renal pelvis (Figure 5). The lesion close to the kidney (described on US) corresponded to an extremely dilated renal pelvis.
3Diagnosis
Rupture of the renal kidney pelvis and the urinoma.
4Discussion
BACKGROUND:
Acute obstructive uropathy is a medical emergency, which is often accompanied by acute renal failure and/or sepsis2,3. Urinary tract obstruction and hydronephrosis can occur for a variety of reasons. The most common acquired causes include nephrolithiasis; ureteropelvic junction stenosis/obstruction; ureteral or urethral stricture; benign prostatic hyperplasia; and urinary trauma. Complications associated with urinary tract obstruction and hydronephrosis depend on the aetiology and duration of insult. Infection and loss of renal function may develop.
THERAPY PLANNING:
The patient underwent aspiration of the subrenal urinoma with insertion of a pigtail drain and nephrostomy tube placement under ultrasonographic guidance. Follow-up US examination demonstrated regression of fluid collections, and the urinary tract was without signs of dilation (Figure 6). On follow-up CT scan (done 4 days after), marked regression of the size of the retroperitoneal urinoma was evident. There was a stone of about 6 mm in diameter located lateral to the ileopsoas muscle in the right pelvis outside the urinary tract.
OUTCOME & PROGNOSIS:
Our final diagnosis was spontaneous rupture of the renal pelvis with subsequent urinoma. The most common cause of spontaneous renal rupture is nephrolithiasis with subsequent luminal obstruction. It is known that the spontaneous passage rate is estimated to be nearly 50 % for stones 5-10 mm in size (dependent on factors such as age, gender and previous stone history). In this case, the cause of rupture was most probably related to compression of the ureter by the preceding abscess of the iliac muscle, and the resulting haematoma. Urinoma resulting from rupture of the renal pelvis is a rare diagnosis. It can also occur as an iatrogenic complication of interventional medical procedures, or, because of blunt or penetrating trauma to the urinary tract.
Acute obstructive uropathy is a medical emergency, which is often accompanied by acute renal failure and/or sepsis2,3. Urinary tract obstruction and hydronephrosis can occur for a variety of reasons. The most common acquired causes include nephrolithiasis; ureteropelvic junction stenosis/obstruction; ureteral or urethral stricture; benign prostatic hyperplasia; and urinary trauma. Complications associated with urinary tract obstruction and hydronephrosis depend on the aetiology and duration of insult. Infection and loss of renal function may develop.
THERAPY PLANNING:
The patient underwent aspiration of the subrenal urinoma with insertion of a pigtail drain and nephrostomy tube placement under ultrasonographic guidance. Follow-up US examination demonstrated regression of fluid collections, and the urinary tract was without signs of dilation (Figure 6). On follow-up CT scan (done 4 days after), marked regression of the size of the retroperitoneal urinoma was evident. There was a stone of about 6 mm in diameter located lateral to the ileopsoas muscle in the right pelvis outside the urinary tract.
OUTCOME & PROGNOSIS:
Our final diagnosis was spontaneous rupture of the renal pelvis with subsequent urinoma. The most common cause of spontaneous renal rupture is nephrolithiasis with subsequent luminal obstruction. It is known that the spontaneous passage rate is estimated to be nearly 50 % for stones 5-10 mm in size (dependent on factors such as age, gender and previous stone history). In this case, the cause of rupture was most probably related to compression of the ureter by the preceding abscess of the iliac muscle, and the resulting haematoma. Urinoma resulting from rupture of the renal pelvis is a rare diagnosis. It can also occur as an iatrogenic complication of interventional medical procedures, or, because of blunt or penetrating trauma to the urinary tract.
5Teaching Points
1. Abdominal ultrasound (US) is typically the first imaging modality used in evaluation of the kidneys and renal collecting system, because it can detect abnormalities such as hydronephrosis, ureteral dilation, and cystic fluid collections in the retroperitoneum.[1]
2. If dilation of the upper urinary tract is detected on ultrasound, a CT scan is usually performed to establish the diagnosis.
2. If dilation of the upper urinary tract is detected on ultrasound, a CT scan is usually performed to establish the diagnosis.
6References
1. Patel K, Batura D. An overview of hydronephrosis in adults. Br J Hosp Med (Lond). 2020 ;81(1):1-8
2. Expert Panel on Interventional Radiology, Scheidt MJ, Hohenwalter EJ, Pinchot JW, et al. ACR appropriateness criteria® radiologic management of urinary tract obstruction. J Am Coll Radiol. 2020; 17(5S): S281-S292
3. Mourmouris PI, Chiras T, Papatsoris AG. Obstructive uropathy: From etiopathology to therapy. World J Nephrol Urol. 2014; 3(1):1-6
2. Expert Panel on Interventional Radiology, Scheidt MJ, Hohenwalter EJ, Pinchot JW, et al. ACR appropriateness criteria® radiologic management of urinary tract obstruction. J Am Coll Radiol. 2020; 17(5S): S281-S292
3. Mourmouris PI, Chiras T, Papatsoris AG. Obstructive uropathy: From etiopathology to therapy. World J Nephrol Urol. 2014; 3(1):1-6

{kind=link}