Vascular CEUS
November 8, 2019
The role of clinical findings in a patient with acute abdominal pain [Feb/Mar 2020]
March 25, 2020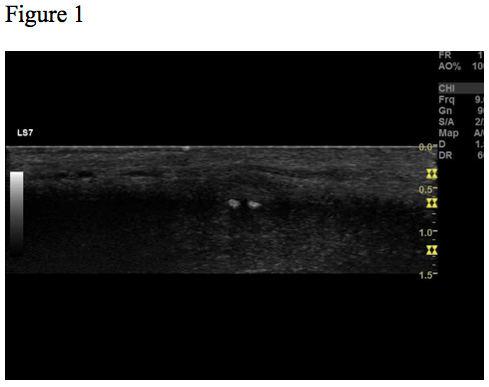
Peyronie’s disease
AUTHORS:
Dilan Yücel Atceken, Department of Radiology, Rigshospitalet, Denmark
Caroline Ewertsen, Department of Radiology, Rigshospitalet, Denmark
Dilan Yücel Atceken, Department of Radiology, Rigshospitalet, Denmark
Caroline Ewertsen, Department of Radiology, Rigshospitalet, Denmark
![Peyronie’s disease </br> [Jan 2020]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/jan2020-fig01.png)
![Peyronie’s disease </br> [Jan 2020]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/jan2020-fig02.png)
![Peyronie’s disease </br> [Jan 2020]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/jan2020-fig03.png)
![Peyronie’s disease </br> [Jan 2020]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/jan2020-fig04.png)
1Case Report
A 55-years old healthy man without any comorbidity had incidentally discovered a lump on the dorsal side of the penis. The lump was painless and did not cause any curving of the penis during erection. On palpation a 0.5 cm subcutaneous lump was discovered. The skin was without discolouration.
Ultrasound examination revealed a 0.6 x 0.4 cm hypoechoic lesion with two hyperechoic spots inside (Fig. 1-3). The lesion was well-circumscribed, located subcutaneously. On elastography, the lesion appeared hard relative to the surrounding tissue (Fig. 4). The lesion was without flow on colour Doppler.
Ultrasound examination revealed a 0.6 x 0.4 cm hypoechoic lesion with two hyperechoic spots inside (Fig. 1-3). The lesion was well-circumscribed, located subcutaneously. On elastography, the lesion appeared hard relative to the surrounding tissue (Fig. 4). The lesion was without flow on colour Doppler.
2Figure Legends
Figure 1, 2, 3 and 4 show the same hypoechoic lesion, a Peyronie’s plaque, in the penile connective tissue. The lesion has a well-defined circumference.
Figure 2. B-mode image. The size and the border of the lesion marked by yellow dotted lines. Lesion measures 0.6 x 0.4 cm.
Figure 3. B-mode image. The lesion contains 2 circular hyperechoic dots, marked with red arrows, which represents calcification with acoustic shadowing, marked with blue arrows.
Figure 4. Elastography image shows that the lesion is harder relative to the surrounding tissue.
Figure 2. B-mode image. The size and the border of the lesion marked by yellow dotted lines. Lesion measures 0.6 x 0.4 cm.
Figure 3. B-mode image. The lesion contains 2 circular hyperechoic dots, marked with red arrows, which represents calcification with acoustic shadowing, marked with blue arrows.
Figure 4. Elastography image shows that the lesion is harder relative to the surrounding tissue.
3Discussion
In 1743 the French surgeon François Gigot de la Peyronie described the above condition, Peyronie disease (PD), also referred to as Induratio Penis Plastica. PD is characterized by the presence of benign fibrotic plaques, Peyronie’s plaques, in the penile connective tissue. More specifically these fibrous plaques are localized in the tunica albuginea surrounding the corpora cavernosa, and often located on the dorsum of the penis. Peyronie’s plaques can be asymptomatic random findings as in the case above, but can also cause pain during coitus, penile deformity and erectile dysfunction, which may cause mental strain.
Ultrasound (US) is a well-established imaging modality for assessing penile diseases due to its’ easy accessibility, painless, non-invasive nature, and exact quantification of Peyronie’s plaques. Another advantage of US is that is does not expose the patient to radiation. Hyperechoic focal thickening of the tunica albuginea is a classic ultrasonographic characteristic of PD. If a plaque is calcified it is seen with acoustic shadowing. In the earlier stages of the disease less characteristic ultrasonographic changes are seen for instance hypoechoic lesions with focal thickening of the paracavernous tissue, echogenic focal thickening of the tunica albuginea and lacking focal continuity of the tunica albuginea.
The pathogenesis is not well established. The main accepted hypothesis is that PD is a result of repetitive micro-trauma against the erect penis, triggering an inflammatory response. These micro-trauma may be unrecognized by the patient. The inflammatory response results in the formation of scar tissue, Peyronie's plaques. As the disease progresses, calcification of the plaques may occur. The fibrous thickening of the tunica albuginea can lead to curvature of the erect penis. 20% of PD patients have Dupuytren’s palmar fibromatosis which may indicate a possible genetic etiological component.
As a differential diagnosis for PD, epitheloid sarcoma may be considered. It is a painless slow-growing soft tissue tumour . Local trauma and thereby scar tissue formation and scleroderma are other possible differential diagnoses.
Ultrasound (US) is a well-established imaging modality for assessing penile diseases due to its’ easy accessibility, painless, non-invasive nature, and exact quantification of Peyronie’s plaques. Another advantage of US is that is does not expose the patient to radiation. Hyperechoic focal thickening of the tunica albuginea is a classic ultrasonographic characteristic of PD. If a plaque is calcified it is seen with acoustic shadowing. In the earlier stages of the disease less characteristic ultrasonographic changes are seen for instance hypoechoic lesions with focal thickening of the paracavernous tissue, echogenic focal thickening of the tunica albuginea and lacking focal continuity of the tunica albuginea.
The pathogenesis is not well established. The main accepted hypothesis is that PD is a result of repetitive micro-trauma against the erect penis, triggering an inflammatory response. These micro-trauma may be unrecognized by the patient. The inflammatory response results in the formation of scar tissue, Peyronie's plaques. As the disease progresses, calcification of the plaques may occur. The fibrous thickening of the tunica albuginea can lead to curvature of the erect penis. 20% of PD patients have Dupuytren’s palmar fibromatosis which may indicate a possible genetic etiological component.
As a differential diagnosis for PD, epitheloid sarcoma may be considered. It is a painless slow-growing soft tissue tumour . Local trauma and thereby scar tissue formation and scleroderma are other possible differential diagnoses.
4Conclusion
Peyronie’s Disease (PD) is a benign disease that often presents with benign fibrotic plaques in the penile connective tissue in asymptomatic or symptomatic patients.
Ultrasound (US) is the primary modality for visualization of the fibrotic penile changes especially due to its easy accessibility, non-invasive and non-radiating nature.
Knowledge of the ultrasonographic features of PD is essential for the diagnosis.
Ultrasound (US) is the primary modality for visualization of the fibrotic penile changes especially due to its easy accessibility, non-invasive and non-radiating nature.
Knowledge of the ultrasonographic features of PD is essential for the diagnosis.
5References
1. Schneider HJ, Rugendorff EW, Röhrborn C. Pathogenesis, diagnosis and therapy of Induratio penis plastica (IPP) Int Urol Nephrol. 1985;17:235–44.
2. Kalokairinou K, Konstantinidis C, Domazou M, et al. US imaging in Peyronie's disease. J Clin Imaging Sci. 2012;2:63–63
3. Kalokairinou K, Konstantinidis C, Domazou M, et al. US imaging in Peyronie's disease. J Clin Imaging Sci. 2012;2:63–63
4. Maitê Aline Vieira Fernandes, Luis Ronan Marquez Ferreira de Souza, and Luciano Pousa Cartafina. Ultrasound evaluation of the penis. Radiol Bras. 2018 Jul-Aug; 51(4): 257–261.
5. Moreland RB, Nehra A. Pathophysiology of Peyronie's disease. Int J Impot Res. 2002 Oct;14(5):406-10.
6. Hatzimouratidis K, Eardley I, Giuliano F, Hatzichristou D, Moncada I, Salonia A, Vardi Y, Wespes E, European Association of Urology, EAU guidelines on penile curvature. Eur Urol 2012;62: 543-52
7. Needs T, Fillman EP. Cancer, Epithelioid Sarcoma. [Updated 2019 Jun 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532911/
8. Kalokairinou K, Konstantinidis C, Domazou M, et al. US imaging in Peyronie's disease. J Clin Imaging Sci. 2012;2:63–63
2. Kalokairinou K, Konstantinidis C, Domazou M, et al. US imaging in Peyronie's disease. J Clin Imaging Sci. 2012;2:63–63
3. Kalokairinou K, Konstantinidis C, Domazou M, et al. US imaging in Peyronie's disease. J Clin Imaging Sci. 2012;2:63–63
4. Maitê Aline Vieira Fernandes, Luis Ronan Marquez Ferreira de Souza, and Luciano Pousa Cartafina. Ultrasound evaluation of the penis. Radiol Bras. 2018 Jul-Aug; 51(4): 257–261.
5. Moreland RB, Nehra A. Pathophysiology of Peyronie's disease. Int J Impot Res. 2002 Oct;14(5):406-10.
6. Hatzimouratidis K, Eardley I, Giuliano F, Hatzichristou D, Moncada I, Salonia A, Vardi Y, Wespes E, European Association of Urology, EAU guidelines on penile curvature. Eur Urol 2012;62: 543-52
7. Needs T, Fillman EP. Cancer, Epithelioid Sarcoma. [Updated 2019 Jun 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK532911/
8. Kalokairinou K, Konstantinidis C, Domazou M, et al. US imaging in Peyronie's disease. J Clin Imaging Sci. 2012;2:63–63

{kind=link}