Peyronie’s disease [Jan 2020]
January 25, 2020CEUS in Liver Imaging
April 8, 2020
The role of clinical findings in a patient with acute abdominal pain
AUTHORS:
Parisa Seyedhosseini and Caroline Ewertsen, Rigshospitalet, Copenhagen University Hospital.
Parisa Seyedhosseini and Caroline Ewertsen, Rigshospitalet, Copenhagen University Hospital.
![The role of clinical findings in a patient with acute abdominal pain </br> [Feb/Mar 2020]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotm_mar2020_1.png)
![The role of clinical findings in a patient with acute abdominal pain </br> [Feb/Mar 2020]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotm_mar2020_2.png)
![The role of clinical findings in a patient with acute abdominal pain </br> [Feb/Mar 2020]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotm_Mar2020_3.png)
![The role of clinical findings in a patient with acute abdominal pain </br> [Feb/Mar 2020]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotm_Mar2020_4.png)
1Clinical history and imaging:
A 56-year-old male was admitted to our hospital because of myocardial infarction and the need for subacute coronary artery bypass grafting (CABG). After 4 days of hospitalization (on the day prior to surgery) the patient suddenly experienced fever (38.3°C), constant and severe pain in the right side of the abdomen and also vomitting.
On palpation the patient had pain in the right upper quadrant and slight tenderness in the right lower quadrant. The laboratory tests showed leucocytosis and elevated CRP, bilirubin, ALT, ALP and LDH.
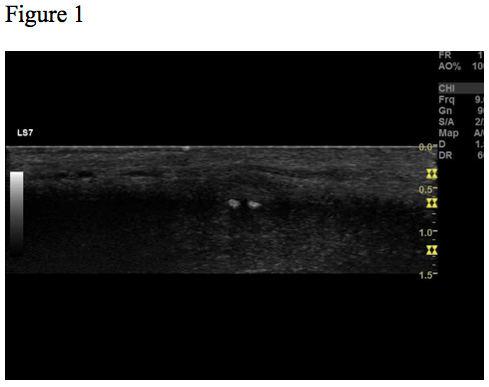
The patient was referred to ultrasound with suspicion of acute cholecystitis as a possible primary diagnosis and acute appendicitis as a secondary possibility. An ultrasound examination of the abdomen was performed using a GE Logiq E9 system with a curved array transducer with a frequency of 1-6 MHz (GE, Chalfont St. Giles). The examination revealed sludge and a stone of approximately 1 cm in the gallbladder. There was no dilatation of the intra- or extrahepatic bile ducts and the gallbladder wall was without thickening (below 3 mm). The other abdominal organs were normal. The appendix could not be seen. Due to the discrepancy between the clinical history, the imaging findings and the planned cardiac surgery the day after, a CT examination was performed to exclude appendicitis. CT showed pericholecystic fat stranding, confirming the diagnosis of cholecystitis. The appendix was located behind the cecum and appeared normal. No other pathology was reported.
Our patient was treated conservatively with intravenous antibiotics, intravenous fluid therapy and analgesics followed by transhepatic gallbladder drainage four days after CT (10 days after symptom onset) in order to decompress the inflamed gallbladder. Conservative treatment was chosen because the cardiac risk for surgery was high due to the recent myocardial infarction.
On palpation the patient had pain in the right upper quadrant and slight tenderness in the right lower quadrant. The laboratory tests showed leucocytosis and elevated CRP, bilirubin, ALT, ALP and LDH.
The patient was referred to ultrasound with suspicion of acute cholecystitis as a possible primary diagnosis and acute appendicitis as a secondary possibility. An ultrasound examination of the abdomen was performed using a GE Logiq E9 system with a curved array transducer with a frequency of 1-6 MHz (GE, Chalfont St. Giles). The examination revealed sludge and a stone of approximately 1 cm in the gallbladder. There was no dilatation of the intra- or extrahepatic bile ducts and the gallbladder wall was without thickening (below 3 mm). The other abdominal organs were normal. The appendix could not be seen. Due to the discrepancy between the clinical history, the imaging findings and the planned cardiac surgery the day after, a CT examination was performed to exclude appendicitis. CT showed pericholecystic fat stranding, confirming the diagnosis of cholecystitis. The appendix was located behind the cecum and appeared normal. No other pathology was reported.
Our patient was treated conservatively with intravenous antibiotics, intravenous fluid therapy and analgesics followed by transhepatic gallbladder drainage four days after CT (10 days after symptom onset) in order to decompress the inflamed gallbladder. Conservative treatment was chosen because the cardiac risk for surgery was high due to the recent myocardial infarction.
2Discussion
Acute cholecystitis is the most common complication to gallstone disease, due to obstruction of the cystic duct. Another irritant may also be required to cause inflammation in the gallbladder. Infection of the bile in the biliary system can in some cases result in cholecystitis. In about 5 to 10 percent of cases, cholecystitis occurs without evidence of gallstones [1].
Different modalities may be used to confirm the diagnosis of cholecystitis before starting treatment. Ultrasound is usually the preferred initial modality. It is readily available, cheaper than CT and scintigraphy and causes no radiation. In addition it is dynamic with the possibility of assessing Murphy’s sign.
In our case, the patient had signs and symptoms compatible with cholecystitis, but ultrasound did not show any wall thickening, only a stone in the gallbladder.
Because the patient was scheduled for cardiac surgery the next day and appendicitis could not be ruled out, the patient underwent CT, which confirmed the clinical suspicion of cholecystitis.
Ultrasound has a very high sensitivity and specificity (> 95%) for the diagnosis of gallstones more than 2 mm in diameter [2], and it is known to be more sensitive than CT. Some reviews find CT more sensitive (85% vs 68%) and (92% vs 79%) for the establishment of the diagnosis of cholecystitis [3,4], although the specificity for both modalities were 100% [3]. Moreover CT is a good modality to evaluate the entire abdomen in one examination. In another review of diagnostic imaging in acute cholecystitis, sensitivity and specificity of ultrasound, MRI and cholescintigraphy were investigated. Scintigraphy was more sensitive than ultrasound, 96% (95%CI: 94%-97%) versus 81% (95%CI: 75%-87%) and MRI, 85% (95%CI: 66%-95%). There was no significant difference in specificity among these modalities [5]. The disadvantage of scintigraphy is its inability to diagnose complications to acute cholecystitis.
Cholecystitis is initially treated by fasting, intravenous fluid therapy, intravenous antibiotics and analgesics. After the initial treatment, cholecystectomy through laparoscopy or open surgery is recommended within 5-7 days after symptom onset.
Patients with a high risk at surgery can be treated by percutanous or endoscopic gallbladder drainage [6].
In our case, the patient had signs and symptoms compatible with cholecystitis, but ultrasound did not show any wall thickening, only a stone in the gallbladder.
Because the patient was scheduled for cardiac surgery the next day and appendicitis could not be ruled out, the patient underwent CT, which confirmed the clinical suspicion of cholecystitis.
Ultrasound has a very high sensitivity and specificity (> 95%) for the diagnosis of gallstones more than 2 mm in diameter [2], and it is known to be more sensitive than CT. Some reviews find CT more sensitive (85% vs 68%) and (92% vs 79%) for the establishment of the diagnosis of cholecystitis [3,4], although the specificity for both modalities were 100% [3]. Moreover CT is a good modality to evaluate the entire abdomen in one examination. In another review of diagnostic imaging in acute cholecystitis, sensitivity and specificity of ultrasound, MRI and cholescintigraphy were investigated. Scintigraphy was more sensitive than ultrasound, 96% (95%CI: 94%-97%) versus 81% (95%CI: 75%-87%) and MRI, 85% (95%CI: 66%-95%). There was no significant difference in specificity among these modalities [5]. The disadvantage of scintigraphy is its inability to diagnose complications to acute cholecystitis.
Cholecystitis is initially treated by fasting, intravenous fluid therapy, intravenous antibiotics and analgesics. After the initial treatment, cholecystectomy through laparoscopy or open surgery is recommended within 5-7 days after symptom onset.
Patients with a high risk at surgery can be treated by percutanous or endoscopic gallbladder drainage [6].
3Conclusion
Ultrasound is the modality of choice to establish the diagnosis of cholecystitis and gall bladder stones in the acute setting. MR has a high sensitivity and specificity, but may not be widely available. It is imortant to remember that acute cholecystitis is mainly a clinical diagnosis based on the patient’s history and clinical findings [6,7].
4Teaching points
This case demonstrates the importance of a good clinical history and the application of different imaging modalities. With persisting clinical suspicion of cholecystitis and unspecific ultrasound findings, MRI or CT and scintigraphy could be helpful in establishing the diagnosis.
5References
1. Salam FZ, Nezam HA. Acute calculous cholecystitis: Clinical features and diagnosis. [updated 2018 nov 8]. Available from: https://www.uptodate.com/contents/treatment-of-acute-calculous-cholecystitis.
2. Trotman BW, Petrella EJ, Soloway RD, Sanchez HM, Morris TA, Miller WT. Evaluation of radiographic lucency or opaqueness of gallstones as a means of identifying cholesterol or pigment stones. Correlation of lucency or opaqueness with calcium and mineral. Gastroenterology. 1975 Jun;68(6):1563-6.
3. Wertz JR, Lopez JM, Olson D, Thompson WM. Comparing the diagnostic accuracy of ultrasound and CT in evaluating acute cholecystitis. AJR Am J Roentgenol. 2018 Aug;211(2):92-7.
4. Fagenholz PJ, Fuentes E, Kaafarani H, Cropano C, King D, de Moya M, et al. Computed tomography is more sensitive than ultrasound for the diagnosis of acute cholecystitis. Surg Infect (Larchmt). 2015 Oct 5;16(5):509-12.
5. Kiewiet JJ, Leeuwenburgh MM, Bipat S, Bossuyt PM, Stoker J, Boermeester MA. A Systematic review and meta-analysis of diagnostic performance of imaging in acute cholecystitis. Radiology. 2012 Sep 1;264(3):708-20.
6. Svendsen LB, Dahl JB, Hillingsø J. Kirurgisk Kompendium Kittelbog. 3rd ed. Denmark: Nyt nordisk forlay arnold busck; 2011. 334-335 p.
7. Yeung SJ, Escalante CP, Gagel RF. Medical care of cancer patients. US: BC decker Inc; 2009. 262 p.
2. Trotman BW, Petrella EJ, Soloway RD, Sanchez HM, Morris TA, Miller WT. Evaluation of radiographic lucency or opaqueness of gallstones as a means of identifying cholesterol or pigment stones. Correlation of lucency or opaqueness with calcium and mineral. Gastroenterology. 1975 Jun;68(6):1563-6.
3. Wertz JR, Lopez JM, Olson D, Thompson WM. Comparing the diagnostic accuracy of ultrasound and CT in evaluating acute cholecystitis. AJR Am J Roentgenol. 2018 Aug;211(2):92-7.
4. Fagenholz PJ, Fuentes E, Kaafarani H, Cropano C, King D, de Moya M, et al. Computed tomography is more sensitive than ultrasound for the diagnosis of acute cholecystitis. Surg Infect (Larchmt). 2015 Oct 5;16(5):509-12.
5. Kiewiet JJ, Leeuwenburgh MM, Bipat S, Bossuyt PM, Stoker J, Boermeester MA. A Systematic review and meta-analysis of diagnostic performance of imaging in acute cholecystitis. Radiology. 2012 Sep 1;264(3):708-20.
6. Svendsen LB, Dahl JB, Hillingsø J. Kirurgisk Kompendium Kittelbog. 3rd ed. Denmark: Nyt nordisk forlay arnold busck; 2011. 334-335 p.
7. Yeung SJ, Escalante CP, Gagel RF. Medical care of cancer patients. US: BC decker Inc; 2009. 262 p.

{kind=link}