Student Image Challenge 111
February 27, 2026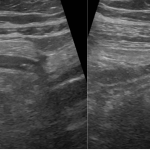
Student Image Challenge 112
March 16, 2026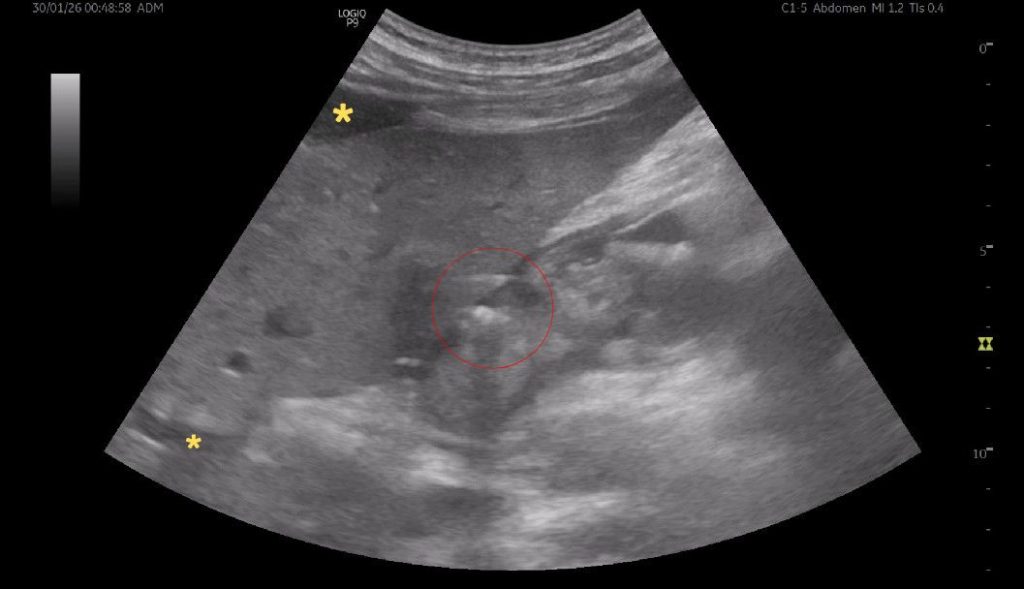
SUBMIT YOUR CASE
EFSUMB invites submission of interesting cases for the website section 'Case of the Month'. All CoM submissions are eligible for selection for free registration at the next Euroson congress. The EFSUMB Publications Committee will review all Best Case of the Month submissions at the end of March 2026. Two cases that receive the most 'likes' over a period from the last congress to March 2026 and judged on a range of factors, including scientific value, will receive free registration for the next EUROSON congress and the third case will receive a cash prize of 100 EUR.
POCUS catches the Breaking point
Authors:
Jovana Tumanov[1], Stefan Pažin[1], Jelena Čavić[1], Nikola Grubor[1], Dragan Vasin[1, 2][1] University Clinical Centre of Serbia, Emergency Radiology Department, Belgrade, Serbia
[2] Faculty of Medicine, University of Belgrade, Serbia

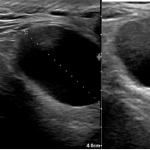
FIGURE 1 and VIDEO 2: Ultrasonography demonstrates the presence of free fluid within the peritoneal recesses, predominantly in the perihepatic and subhepatic regions (yellow asterisks). The fluid appears mildly echogenic, suggestive of inflammatory exudate rather than simple transudate. The duodenal bulb (D1 segment) is thickened and edematous. The area outlined in red demonstrates multiple hyperechoic foci with reverberation artifacts consistent with extraluminal free gas, adjacent to a focal mucosal wall defect. These findings are highly suggestive of a perforated duodenal ulcer.
FIGURE 1 and VIDEO 2: Ultrasonography demonstrates the presence of free fluid within the peritoneal recesses, predominantly in the perihepatic and subhepatic regions (yellow asterisks). The fluid appears mildly echogenic, suggestive of inflammatory exudate rather than simple transudate.
The duodenal bulb (D1 segment) is thickened and edematous. The area outlined in red demonstrates multiple hyperechoic foci with reverberation artifacts consistent with extraluminal free gas, adjacent to a focal mucosal wall defect. These findings are highly suggestive of a perforated duodenal ulcer.


FIGURE 4: Axial contrast-enhanced CT reveals a focal defect of the anterior duodenal wall (blue arrow), with adjacent extraluminal free gas in the hepatoduodenal ligament. Associated free intraperitoneal fluid is noted within the peritoneal recesses (yellow asterisks). These findings are highly suggestive of perforated duodenal ulcer.
FIGURE 3: CT axial-plane (lung window setting) demonstrates extraluminal free gas within the anterior abdominal wall, in the prehepatic region (black arrows), indicative of gastrointestinal perforation.
FIGURE 4: Axial contrast-enhanced CT reveals a focal defect of the anterior duodenal wall (blue arrow), with adjacent extraluminal free gas in the hepatoduodenal ligament. Associated free intraperitoneal fluid is noted within the peritoneal recesses (yellow asterisks). These findings are highly suggestive of perforated duodenal ulcer.
This case highlights the role of point-of-care ultrasound (POCUS) in early detection. Ultrasound showed free fluid, duodenal wall thickening, and hyperechoic foci at the mucosal defect. Findings were confirmed by CT and surgery, enabling timely repair and emphasizing ultrasound’s value in acute emergencies.
Perforation is the most serious complication of peptic ulcer and may also be the first definite evidence of ulceration. It is a life-threatening condition with high morbidity and mortality, particularly when the diagnosis is delayed. Duodenal ulcers, typically affecting the anterior bulb due to gastric acid exposure, are prone to perforation, a life-threatening condition requiring urgent intervention. Anatomically the anterior wall is more exposed to the general peritoneal cavity than is the posterior wall. Although CT remains the gold standard for suspected perforation, demonstrating extraluminal air, free fluid, and wall defects, point-of-care ultrasound (POCUS) provides a rapid bedside alternative capable of detecting subtle early signs.
Recognition of duodenal perforation on ultrasound relies on direct and indirect signs. Indirect signs include localized extraluminal fluid or gas, often pooling near the liver adjacent to the thickened duodenal bulb. Direct signs include hyperechoic foci with reverberation artifacts at the site of perforation.
Detection may be challenging, especially in elderly or immunocompromised patients, or when ultrasound is limited by body habitus or overlying bowel gas. Isolated echogenic free fluid is non-specific, and intraperitoneal air can be misinterpreted as intraluminal gas or artifacts. Therefore, findings must be interpreted in the full clinical context and, when indicated, confirmed with cross-sectional imaging.
Differential diagnoses include acute pancreatitis, perforated gastric ulcer, intestinal obstruction, mesenteric ischemia, appendicitis, and diverticulitis. Accurate diagnosis depends on recognizing the constellation of turbid peritoneal fluid, bowel wall edema, and extraluminal gas, which strongly suggests duodenal perforation.
THERAPY PLANNING:
In this case, the ultrasound findings were confirmed by CT examination and verified surgically, demonstrating a perforated anterior duodenal bulb ulcer with peritonitis. Management of duodenal bulb perforation is primarily surgical, involving closure of the mucosal defect, peritoneal lavage, and drainage of dependent spaces. Prompt intervention is critical to prevent ongoing peritoneal contamination, sepsis, and multi-organ failure.
PROGNOSIS:
Prognosis of perforated duodenal ulcer largely depends on early diagnosis and prompt surgical intervention. Timely management is associated with favorable outcomes, whereas delayed treatment significantly increases the risk of diffuse peritonitis, sepsis, multi-organ failure, and mortality. Advanced age, comorbidities, and hemodynamic instability are major adverse prognostic factors.
2. Diagnostic pitfalls: Ultrasound may be limited by subtle findings, isolated fluid, misinterpreted intraluminal gas, or patient habitus; clinical context and confirmatory CT are essential to avoid misdiagnosis.
3. Imaging-Guided Management: Combining POCUS with CT and surgical assessment allows rapid diagnosis and operative planning, improving patient outcomes in life-threatening gastrointestinal perforations.
2. Romano S, Somma C, Sciuto A, Jutidamrongphan W, Pacella D, Esposito F, et al. MDCT Findings in Gastrointestinal Perforations and the Predictive Value according to the Site of Perforation. Tomography. 2022;8(2):667 687. doi:10.3390/tomography8020056
3. Goudie A. Detection of intraperitoneal free gas by ultrasound. Australas J Ultrasound Med. 2013;16(2):56 61. doi:10.1002/j.2205 0140.2013.tb00166.x

{kind=link}