
Atypical CEUS Pattern as a Diagnostic Clue in a Focal Liver Lesion [February 2026]
March 30, 2026
Student Image Challenge 113
May 20, 2026
SUBMIT YOUR CASE
EFSUMB invites submission of interesting cases for the website section 'Case of the Month'. All CoM submissions are eligible for selection for free registration at the next Euroson congress. The EFSUMB Publications Committee will review all Best Case of the Month submissions at the end of March 2026. Two cases that receive the most 'likes' over a period from the last congress to March 2026 and judged on a range of factors, including scientific value, will receive free registration for the next EUROSON congress and the third case will receive a cash prize of 100 EUR.
Hepatic Hemangiomas Associated with Cutaneous Infantile Hemangiomas: An Ultrasound Case Study
Authors:
MD Nis Elbrønd Larsen[1], MD Arne Hørlyck[1], MD PhD Sheyanth Mohanakumar[1][1] Department of Radiology, Aarhus University Hospital, Aarhus, Denmark






1Clinical History
A two-month-old girl (born at gestational age 36+0 weeks) was referred for abdominal ultrasound to rule out infantile hepatic hemangiomas (HH) due to an increasing number of small cutaneous infantile hemangiomas (CIH). There is a known association between multiple or large CIH and visceral hemangiomas, including HH (1+3). In total, 10 CIH were identified, the largest measuring 1 cm in diameter. The patient had also been diagnosed with an atrial septal defect (secundum type), detected during evaluation of a heart murmur. Otherwise, the girl was healthy and thriving. An abdominal sonography was performed using a LOGIQ E10 ultrasound system (GE Healthcare, Chicago, IL, USA) with a high-frequency probe (ML 4-20-D).
2Image Findings
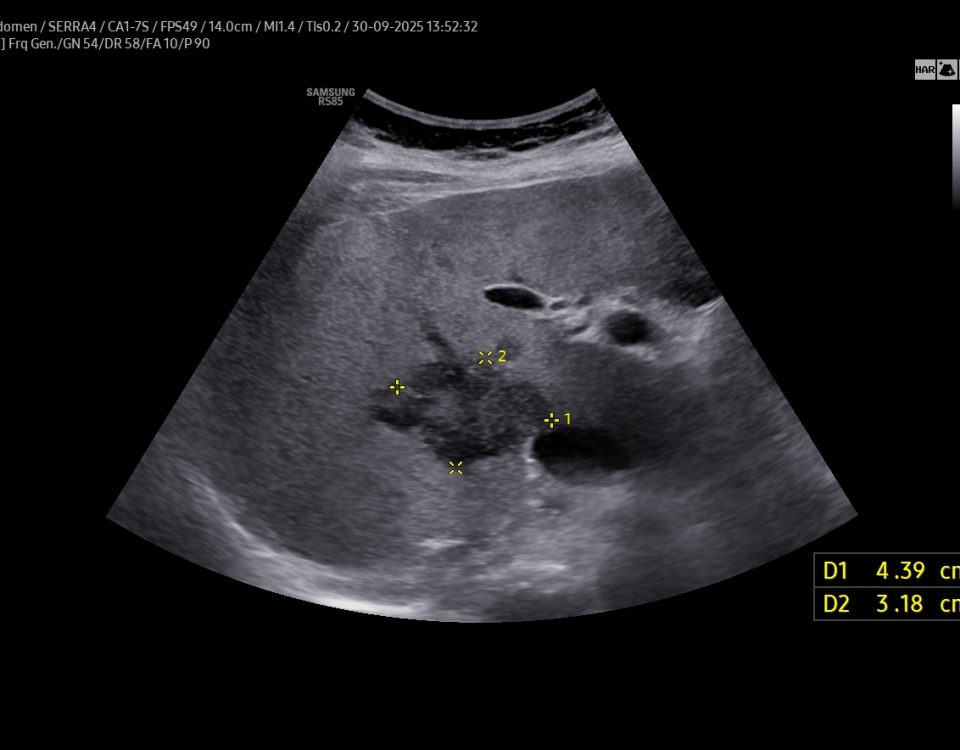
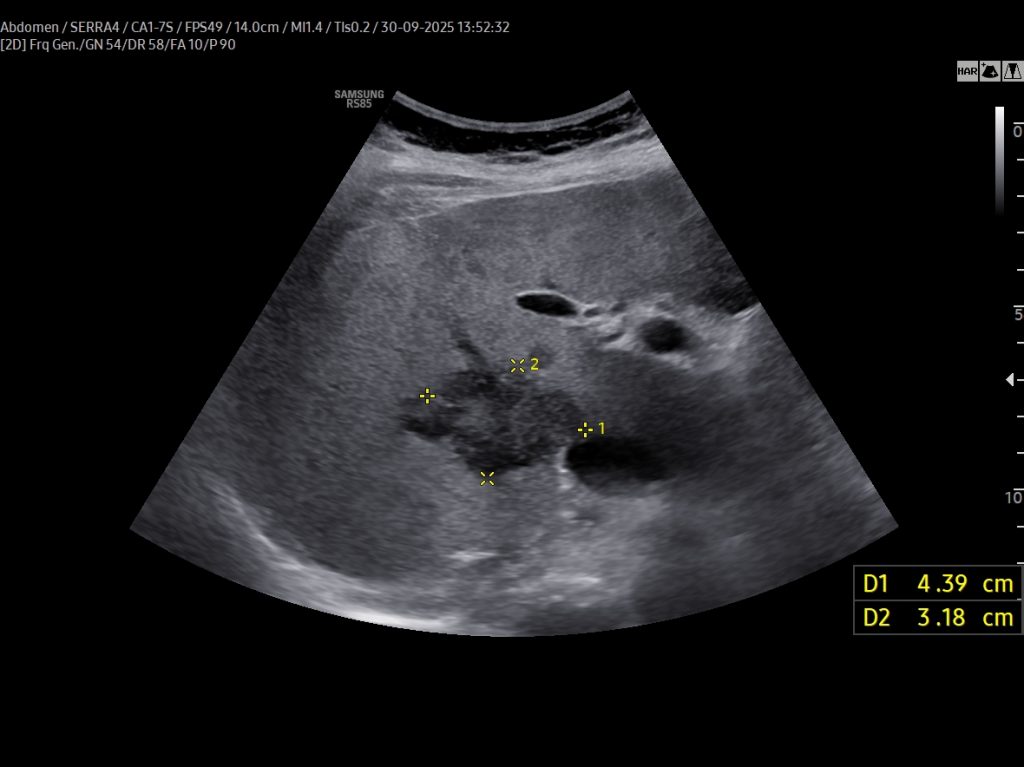
A: B-Mode image in the axial plane demonstrating multiple hyperechoic, well-defined lesions in the liver. Other lesions demonstrate a hypoechoic central area.
B: Doppler image of capillary hemangioma located ventrally in the right hepatic lobe, demonstrating large, tortuous vessels suggestive of possible arteriovenous shunting.
C: Triplex Doppler image of the portal vein demonstrating flow velocities of approximately 37cm/s.
D: Triplex Doppler image of a hepatic vein demonstrating a normal triphasic flow pattern.
E: B-mode image in the coronal plane, showing a slightly heterogeneous lesion in the spleen, most consistent with a splenic hemangioma.
F 1-3: Axial B-mode images from the initial examination and follow-up scans at approximately 4 and 12 weeks, demonstrating shrinkage of a monitored hepatic hemangioma from 12 mm initially to 9 mm and finally 6 mm.
B: Doppler image of capillary hemangioma located ventrally in the right hepatic lobe, demonstrating large, tortuous vessels suggestive of possible arteriovenous shunting.
C: Triplex Doppler image of the portal vein demonstrating flow velocities of approximately 37cm/s.
D: Triplex Doppler image of a hepatic vein demonstrating a normal triphasic flow pattern.
E: B-mode image in the coronal plane, showing a slightly heterogeneous lesion in the spleen, most consistent with a splenic hemangioma.
F 1-3: Axial B-mode images from the initial examination and follow-up scans at approximately 4 and 12 weeks, demonstrating shrinkage of a monitored hepatic hemangioma from 12 mm initially to 9 mm and finally 6 mm.
3Diagnosis
Multiple hepatic lesions were identified on ultrasound (A). Some lesions appeared as typical, well-defined hyperechoic cavernous hemangiomas (2), while others demonstrated large, tortuous vessels. Additional lesions showed a hyperechoic rim with a hypoechoic center and internal Doppler flow, consistent with capillary hemangiomas (2). In some HH (B), arteriovenous shunting was suspected. However, Triplex Doppler examination demonstrated normal hepatoportal flow in the portal vein (C) with flow velocities below 40 cm/s – within the normal range for the age – as well as a normal triphasic flow pattern in the hepatic veins (D).
A lesion with heterogeneous echogenicity – most consistent with a splenic hemangioma- was also identified in the spleen (E). Follow-up ultrasound examination demonstrated rapid regression of the HH (F2-3).
4Discussion
An association exists between large or multiple CIH and HH (1+3). HH may lead to hepatomegaly, abnormal liver function, coagulopathy, arteriovenous shunting, and congestive heart failure, which in severe cases may be life-threatening. Therefore, screening for visceral hemangiomas with abdominal ultrasound has been recommended in cases presenting with 5 or more CIH (3).
In the present case, multiple hemangiomas – both cavernous and capillary subtypes - were detected in both liver and spleen. Some of the hepatic lesions demonstrated features suggestive of arteriovenous shunting.
Treatment with propranolol (Hemangiol) has evolved as the first-line treatment for infantile hemangiomas (3). Treatment was considered following the first ultrasound but was deferred because the infant was clinically well, showed no sign of high-output cardiac failure or steal phenomenon, and the CIH were already demonstrating spontaneous regression in both size and numbers.
Follow-up ultrasound exams showed significant reduction in the HH's size and number, supporting a conservative management strategy for this clinically stable patient.
Additional imaging techniques like magnetic resonance imaging (MRI) or contrast-enhanced ultrasound (CEUS) can help further characterize liver vascular lesions when diagnosis is uncertain. However, in this case, the ultrasound results, along with the clinical context of multiple CIH and the benign clinical progression, were deemed sufficiently distinctive, so no further imaging was necessary.
In the present case, multiple hemangiomas – both cavernous and capillary subtypes - were detected in both liver and spleen. Some of the hepatic lesions demonstrated features suggestive of arteriovenous shunting.
Treatment with propranolol (Hemangiol) has evolved as the first-line treatment for infantile hemangiomas (3). Treatment was considered following the first ultrasound but was deferred because the infant was clinically well, showed no sign of high-output cardiac failure or steal phenomenon, and the CIH were already demonstrating spontaneous regression in both size and numbers.
Follow-up ultrasound exams showed significant reduction in the HH's size and number, supporting a conservative management strategy for this clinically stable patient.
Additional imaging techniques like magnetic resonance imaging (MRI) or contrast-enhanced ultrasound (CEUS) can help further characterize liver vascular lesions when diagnosis is uncertain. However, in this case, the ultrasound results, along with the clinical context of multiple CIH and the benign clinical progression, were deemed sufficiently distinctive, so no further imaging was necessary.
5Teaching Points
• Screening for hepatic and other visceral hemangiomas: Infants presenting with large or multiple CIH should be screened for hepatic or other visceral hemangiomas due to the potential risk of significant morbidity and, in severe cases, mortality.
• Comprehensive hemodynamic assessment with Doppler and Triplex Ultrasound: Hepatic hemangiomas and the hepatic vasculature should be evaluated using Doppler and Triplex ultrasound to assess for possible arteriovenous shunting and hemodynamic consequences.
• Potential for spontaneous regression: Visceral hemangiomas may demonstrate rapid spontaneous regression, even in the absence of medical treatment, highlighting the importance of careful clinical and ultrasound follow-up.
• Comprehensive hemodynamic assessment with Doppler and Triplex Ultrasound: Hepatic hemangiomas and the hepatic vasculature should be evaluated using Doppler and Triplex ultrasound to assess for possible arteriovenous shunting and hemodynamic consequences.
• Potential for spontaneous regression: Visceral hemangiomas may demonstrate rapid spontaneous regression, even in the absence of medical treatment, highlighting the importance of careful clinical and ultrasound follow-up.
6References
1. Hughes JA, Hill V, Patel K, Syed S, Harper J, De Bruyn R. Cutaneous haemangioma: prevalence and sonographic characteristics of associated hepatic haemangioma. Clin Radiol. 2004;59(3):273-280. doi:10.1016/S0009-9260(03)00267-8
2. Kacała A, Dorochowicz M, Matus I, et al. Hepatic Hemangioma: Review of Imaging and Therapeutic Strategies. Medicina (Kaunas). 2024;60(3):449. Published 2024 Mar 8. doi:10.3390/medicina60030449
3. Lewis D, Vaidya R. Congenital and Infantile Hepatic Hemangioma. [Updated 2023 Jun 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK518988/
2. Kacała A, Dorochowicz M, Matus I, et al. Hepatic Hemangioma: Review of Imaging and Therapeutic Strategies. Medicina (Kaunas). 2024;60(3):449. Published 2024 Mar 8. doi:10.3390/medicina60030449
3. Lewis D, Vaidya R. Congenital and Infantile Hepatic Hemangioma. [Updated 2023 Jun 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK518988/
{kind=link}