Student Image Challenge 105
May 7, 2024
Student Image Challenge 106
May 16, 2024
SUBMIT YOUR CASE
EFSUMB invites submission of interesting cases for the website section 'Case of the Month'. All CoM submissions are eligible for selection for free registration at the next Euroson congress. Two cases that receive the most 'likes' in a year will receive free registration for the next EUROSON congress and the third most liked liked case will receive a cash prize of 100 EUR.
Amoebic Liver Necrosis in Contrast-Enhanced Ultrasound
Authors: Ehsan Safai Zadeh, M.D., and Helmut Prosch, M.D.
– Department of Biomedical Imaging and Image-Guided Therapy, Medical University of Vienna, Vienna General Hospital, Vienna, Austria.
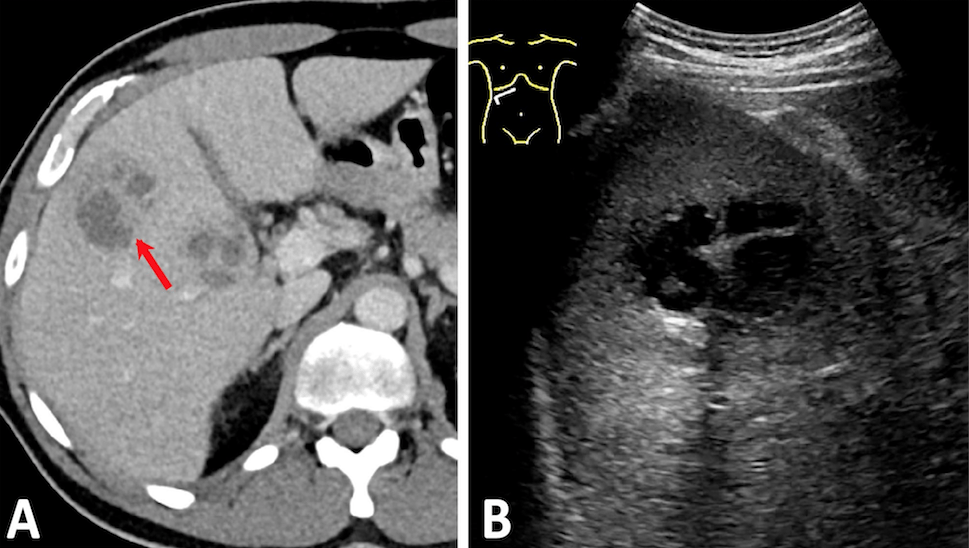
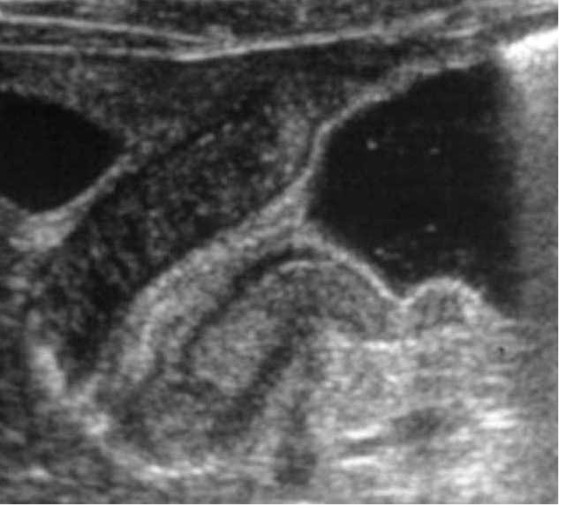
Figure 1: A 44-year-old male patient presented with infectious liver lesions due to amoebic infection in CT (A) and B-mode ultrasound (B). On contrast-enhanced ultrasound, the lesions consistently showed a predominant absence of enhancement throughout the examination, with no rim enhancement in the arterial phase (C) or perilesional wash-out in the portal venous phase (D). The septa exhibited contrast enhancement.
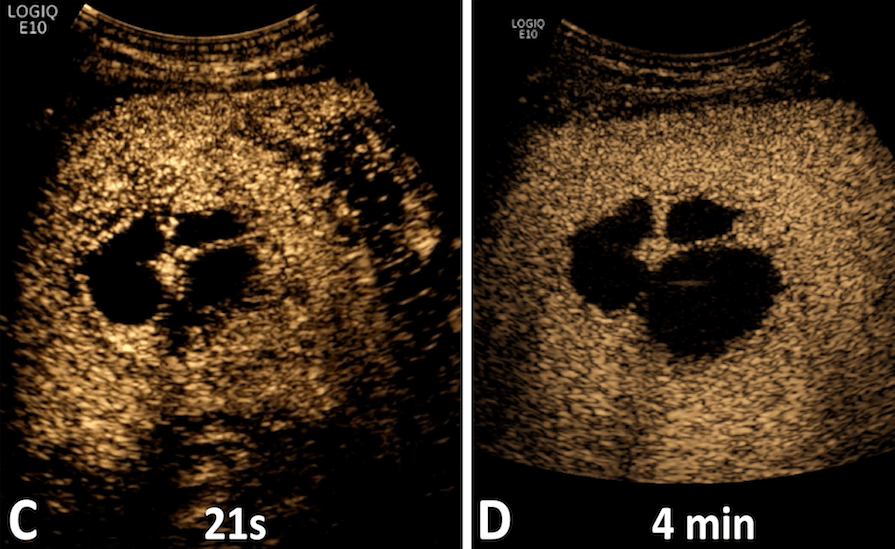
Figure 1: A 44-year-old male patient presented with infectious liver lesions due to amoebic infection in CT (A) and B-mode ultrasound (B). On contrast-enhanced ultrasound, the lesions consistently showed a predominant absence of enhancement throughout the examination, with no rim enhancement in the arterial phase (C) or perilesional wash-out in the portal venous phase (D). The septa exhibited contrast enhancement.
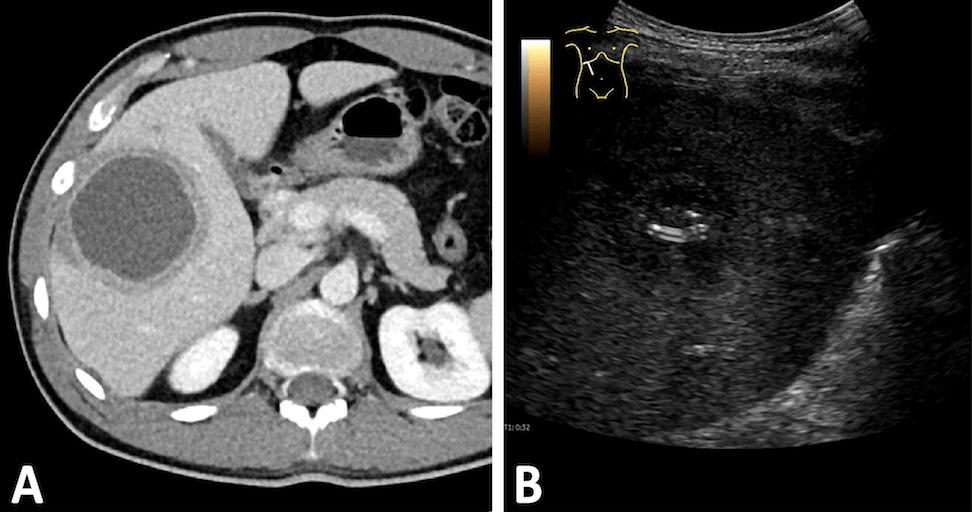
Figure 2: A 31-year-old male patient with cytologically confirmed streptococcal infection seen in CT (A) and B-mode ultrasound (B). On contrast-enhanced ultrasound (CEUS), the lesions consistently showed a central absent enhancement, with rim enhancement in the arterial phase (C) und perilesional wash-out in the portal venous phase (D).
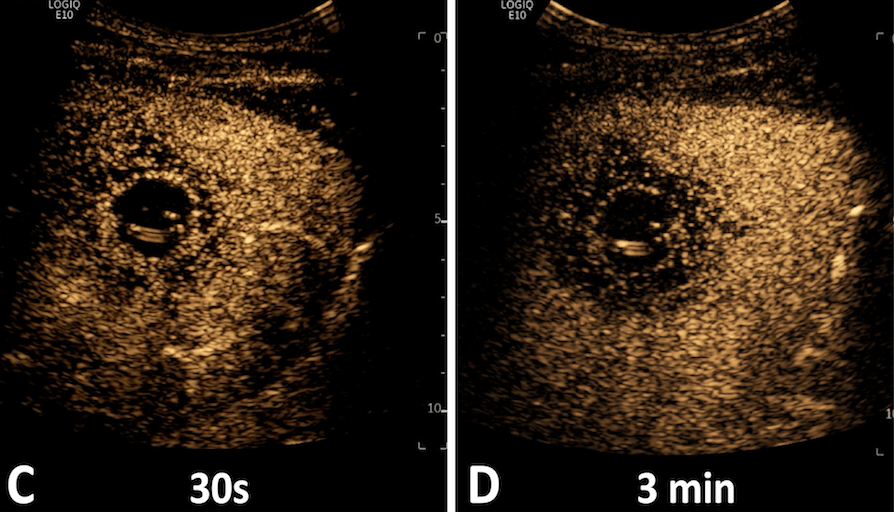
Figure 2: A 31-year-old male patient with cytologically confirmed streptococcal infection seen in CT (A) and B-mode ultrasound (B). On contrast-enhanced ultrasound (CEUS), the lesions consistently showed a central absent enhancement, with rim enhancement in the arterial phase (C) und perilesional wash-out in the portal venous phase (D).
-Unlike pyogenic abscesses (Fig 2), these lesions do not show pronounced rim enhancement or wash-out phenomena on CEUS, which would indicate inflammatory obstruction of the portal vein branches in pyogenic abscesses.
- The term "liver abscess" refers to a collection of pus (neutrophil granulocytes) in the liver and should not be applied to infectious amoebic lesions. Instead, "amoebic necrosis" is the preferred nomenclature. A therapeutic evacuation of the lesion is not necessary.
2. Sayek I, Onat D. Pyogenic and amebic liver abscess. In: Holzheimer RG, Mannick JA, editors. Surgical Treatment: Evidence-Based and Problem-Oriented. Munich: Zuckschwerdt; 2001.
3. Meister P, Irmer H, Paul A, Hoyer DP. Therapy of pyogenic liver abscess with a primarily unknown cause. Langenbecks Arch Surg. 2022; 407(6): 2415-2422.

{kind=link}