Student Image Challenge 93
June 7, 2021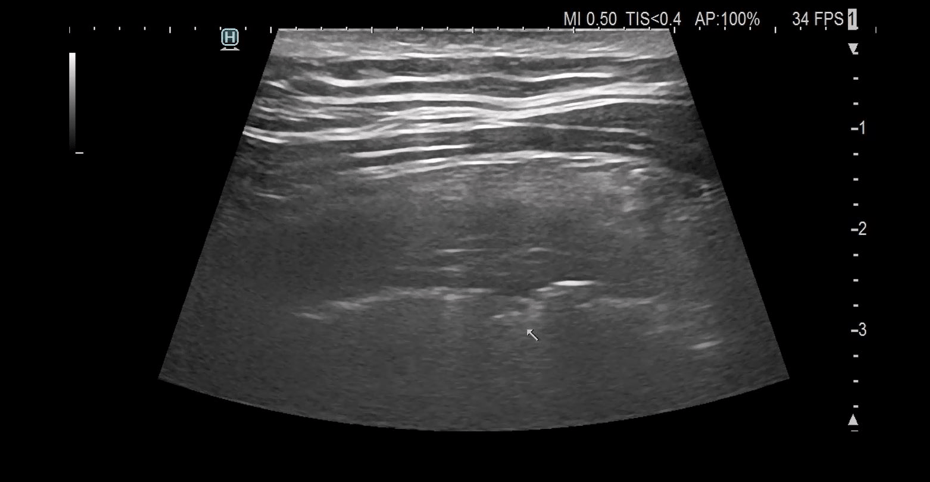
Ultrasound findings in Sars-Cov2-Infection of the lung [August 2021]
July 30, 2021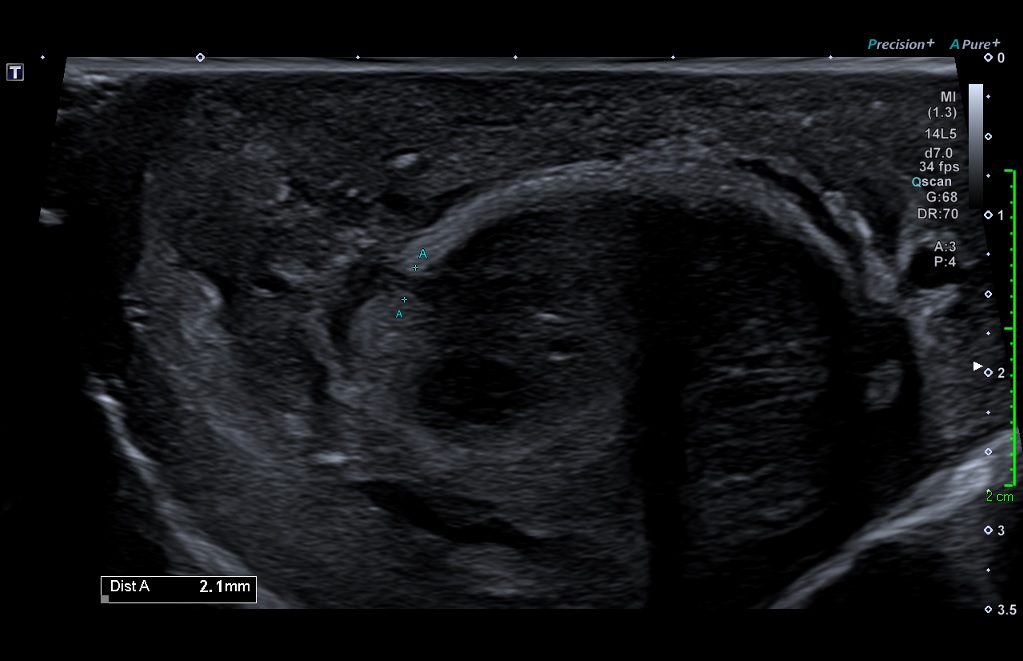
An unusual penile swelling
AUTHORS
Dr Joseph Flexen, Radiology Registrar
Mr Selvakumar Balaraman, Sonographer
Imaging Department, Imperial College Healthcare NHS Trust, London
Dr Joseph Flexen, Radiology Registrar
Mr Selvakumar Balaraman, Sonographer
Imaging Department, Imperial College Healthcare NHS Trust, London
1Clinical history
A 39 year-old male presented to the emergency department with penile swelling and pain. 11 days earlier he had self-injected prostaglandin E1 into the right side of his penis for management of erectile dysfunction (for which he was self-medicating). He reported resistance when injecting, requiring withdrawal and re-puncture. He subsequently noticed a hard lump at the injection site, with increasing pain and swelling. He was initially given antibiotics for a presumed abscess but re-presented to the emergency department as the lump began discharging.
There was no other relevant past medical history.
The patient was febrile and tachycardic. Bloods revealed raised inflammatory markers (neutrophils 8 x 10⁹/L, c-reactive protein 250mg/L). On examination, the penis was grossly swollen with induration on the right side of the shaft. There was a firm right-sided mid-shaft mass, which was actively discharging.
There was no other relevant past medical history.
The patient was febrile and tachycardic. Bloods revealed raised inflammatory markers (neutrophils 8 x 10⁹/L, c-reactive protein 250mg/L). On examination, the penis was grossly swollen with induration on the right side of the shaft. There was a firm right-sided mid-shaft mass, which was actively discharging.
2Imaging findings
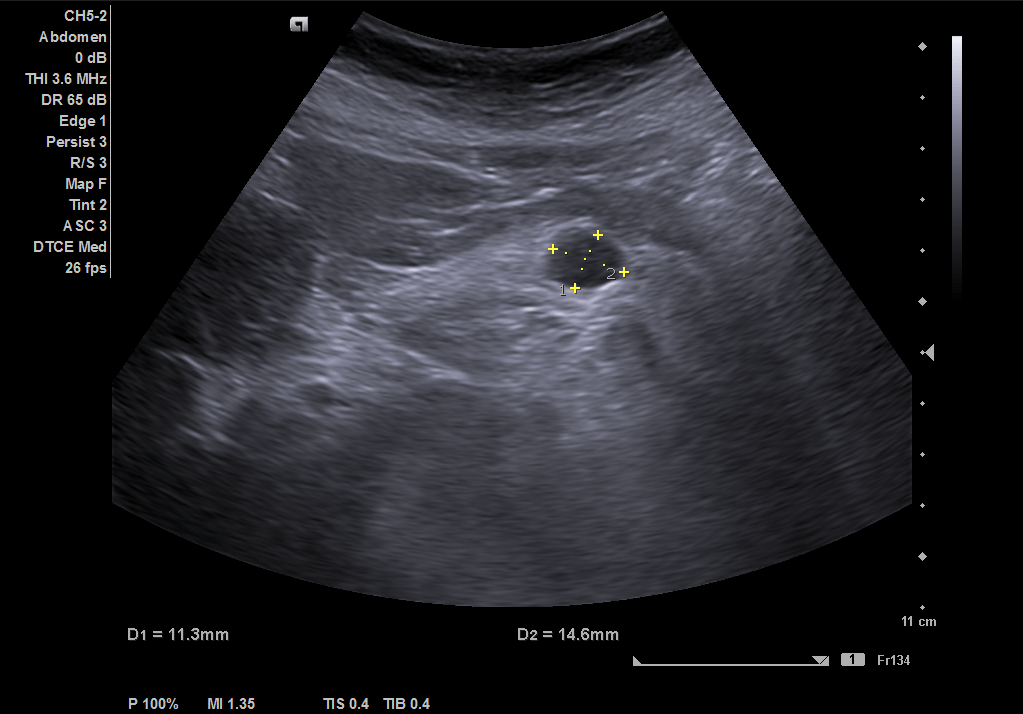
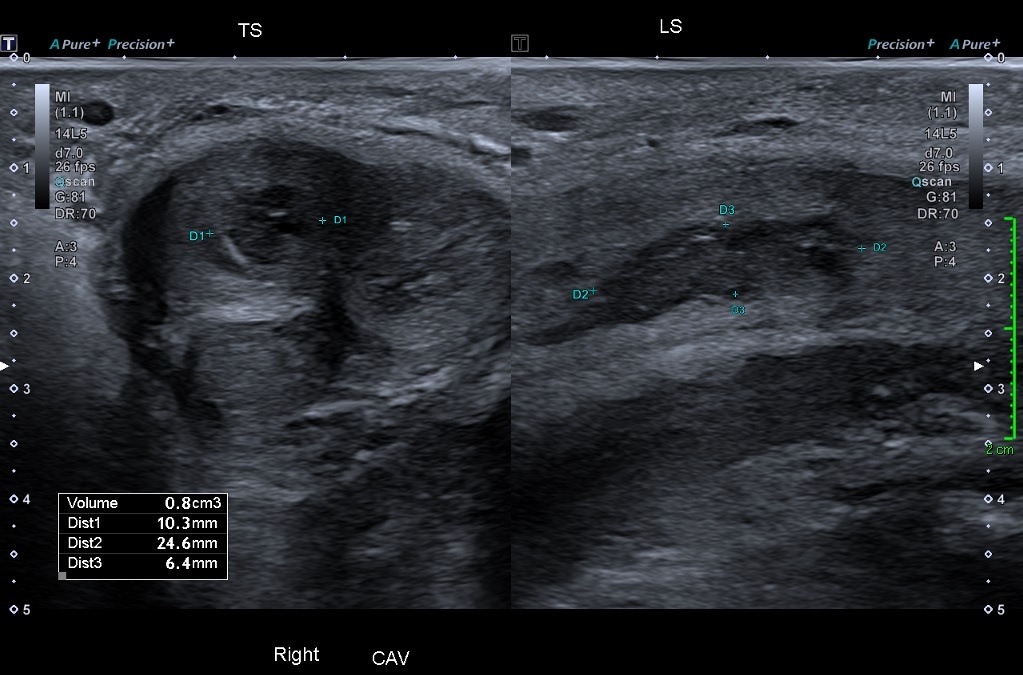
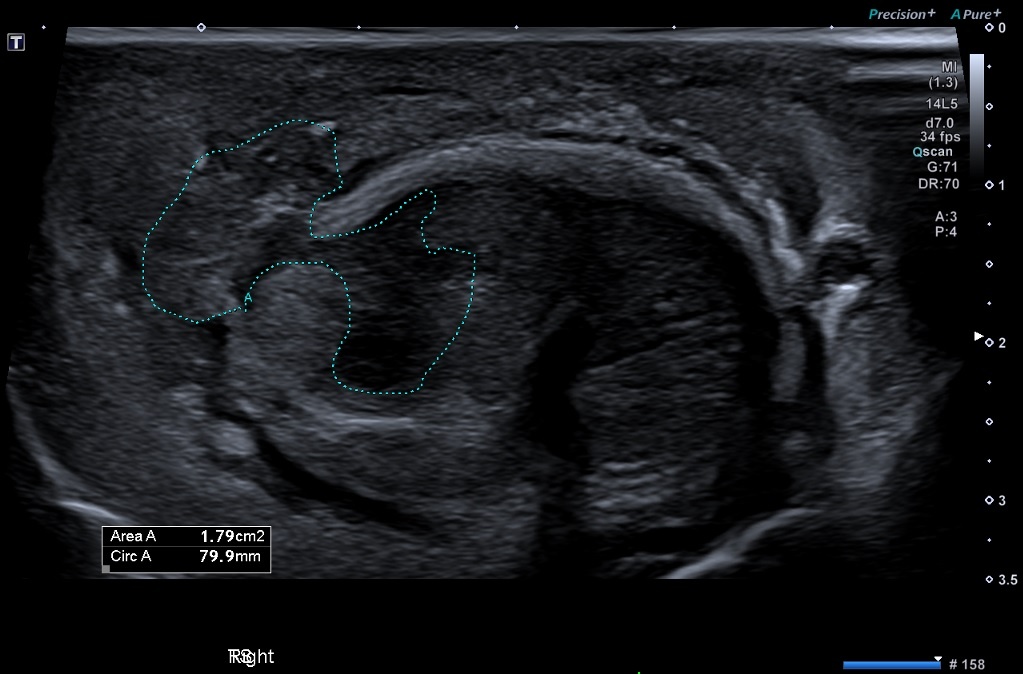
Initial ultrasound showed a discontinuity in the right lateral aspect of the corpora cavernosum along the mid-shaft (Figure 1) There was an associated hypoechoic collection measuring 10 x 25 x 6mm, with intra and extracavernosal components. (Figures 2 & 3) There was extensive surrounding inflammatory change.
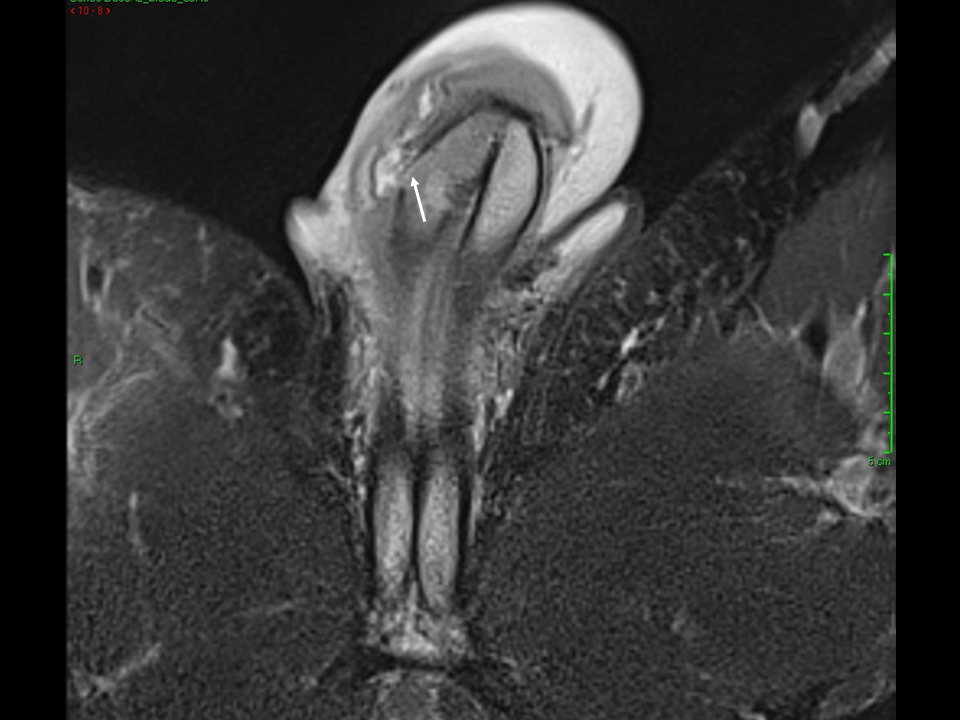
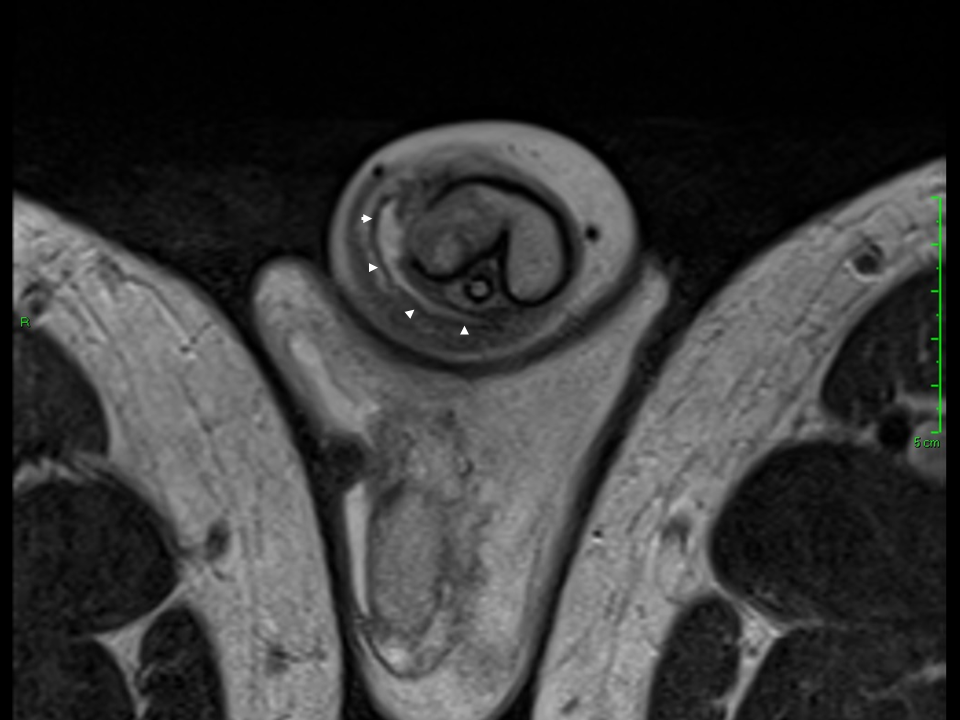
An MRI the same day again demonstrated a defect in the tunica albuginea of the right corpus cavernosum (arrow) and associated communicating intra and extra cavernosal collection (arrow heads) (Figures 4 & 5).
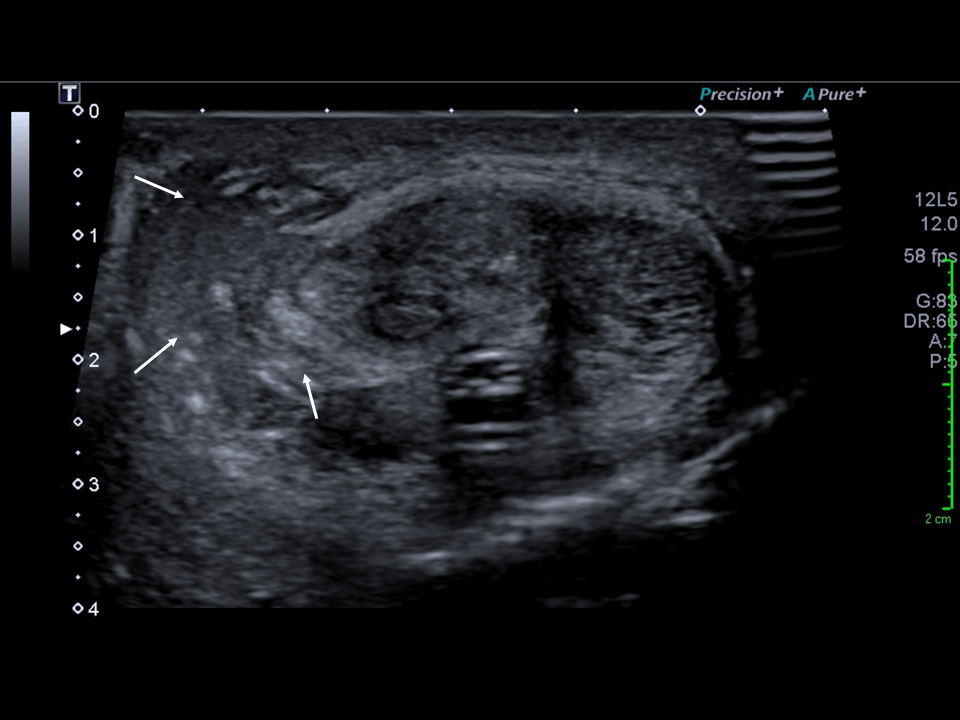
After 5 days of intravenous antibiotics, a further ultrasound was performed. It showed overall reduction in generalised oedema but relatively unchanged appearance of the cavernosal collection. (arrows) (Figure 6).
The patient went on to have an exploration with incision and drainage of the cavernosal collection.
An MRI the same day again demonstrated a defect in the tunica albuginea of the right corpus cavernosum (arrow) and associated communicating intra and extra cavernosal collection (arrow heads) (Figures 4 & 5).
After 5 days of intravenous antibiotics, a further ultrasound was performed. It showed overall reduction in generalised oedema but relatively unchanged appearance of the cavernosal collection. (arrows) (Figure 6).
The patient went on to have an exploration with incision and drainage of the cavernosal collection.
3Diagnosis
IIntra and extracavernosal abscess secondary to prostaglandin E1 injection.
4Discussion
Erectile dysfunction is defined as the persistent inability to attain and/or maintain an erection. Studies suggest a worldwide prevalence of between 19-52%. (1) Of these men, 90% have an organic cause, including cardiovascular disease, diabetes mellitus, hormonal disorders, neurological disorders and anatomical abnormalities. The remaining 10% are psychogenic in nature. (1)
Conservative treatment strategies aim to address the underlying risk factors including lifestyle advice (alcohol reduction, avoiding recreational drugs, psychosexual counselling etc.). The first-line pharmacological treatments are phosphodiesterase type-5 inhibitors, which are taken per orally. Second-line treatments include vacuum erection assistance devices, medicated urethral system for erection and intracavernous injection of prostaglandin E1. (2)
These are not without risk however and complications do occur. With regards to intracavernous injection, complications include infection, haematoma, needle breakage and fibrosis. (3-5) With regards to infection, this is reported as between 1 in 50 – 1 in 250 users. (5) Imaging has an important role to play in the accurate diagnosis and management planning of these penile injuries. The most common and probably most accessible first-line modality is ultrasonography, followed by magnetic resonance imaging. (5,6)
This case illustrates the importance of imaging in contributing to the overall patient care and the importance of good communication between radiologists and clinicians cannot be stressed enough. The ability to provide meaningful interpretation of imaging studies relies on the training and experience of the operator. An understanding of the sonographic appearances of penile injury could aid earlier diagnosis and expedite any necessary further management. It is therefore imperative that sonographers and radiologists gain as much exposure to imaging penile injuries as possible, given these are less common than many other traumatic injuries.
Conservative treatment strategies aim to address the underlying risk factors including lifestyle advice (alcohol reduction, avoiding recreational drugs, psychosexual counselling etc.). The first-line pharmacological treatments are phosphodiesterase type-5 inhibitors, which are taken per orally. Second-line treatments include vacuum erection assistance devices, medicated urethral system for erection and intracavernous injection of prostaglandin E1. (2)
These are not without risk however and complications do occur. With regards to intracavernous injection, complications include infection, haematoma, needle breakage and fibrosis. (3-5) With regards to infection, this is reported as between 1 in 50 – 1 in 250 users. (5) Imaging has an important role to play in the accurate diagnosis and management planning of these penile injuries. The most common and probably most accessible first-line modality is ultrasonography, followed by magnetic resonance imaging. (5,6)
This case illustrates the importance of imaging in contributing to the overall patient care and the importance of good communication between radiologists and clinicians cannot be stressed enough. The ability to provide meaningful interpretation of imaging studies relies on the training and experience of the operator. An understanding of the sonographic appearances of penile injury could aid earlier diagnosis and expedite any necessary further management. It is therefore imperative that sonographers and radiologists gain as much exposure to imaging penile injuries as possible, given these are less common than many other traumatic injuries.
5Teaching point/Conclusion:
• Gain an awareness of potential complications of intracavernous injections for erectile dysfunction.
• Understand the key radiological features of such complications.
• Understand the key radiological features of such complications.
6References
1. Hackett G, Kirby M, Wylie K, et al. British Society for Sexual Medicine Guidelines on the Management of Erectile Dysfunction in Men-2017. J Sex Med 2018;15:430-457
2. Hatzimouratidis K, Amar E, Eardley I, Giuliano F, Hatzichristou D, Montorsi F, Vardi Y, Wespes E; European Association of Urology. Guidelines on male sexual dysfunction: erectile dysfunction and premature ejaculation. Eur Urol. 2010 May;57(5):804-14. doi: 10.1016/j.eururo.2010.02.020. Epub 2010 Feb 20. PMID: 20189712.
3. He L, Wen J, Jiang X, Chen H, Tang Y. Long-term efficacy and safety of self-intracavernous injection of prostaglandin E1 for treatment of erectile dysfunction in China. Andrologia. 2011 Jun;43(3):208-12. doi: 10.1111/j.1439-0272.2010.01091.x. Epub 2011 Mar 25. PMID: 21486416.
4. British Association of Urological Surgeons. Penile injection for erection. [Online]. [Accessed 23 August 2020]. Available from http://www.baus.org.uk
5. Moemen MN, Hamed HA, Kamel II, Shamloul RM, Ghanem HM. Clinical and sonographic assessment of the side effects of intracavernous injection of vasoactive substances. Int J Impot Res. 2004 Apr;16(2):143-5. doi: 10.1038/sj.ijir.3901194. PMID: 15014552.
6. Cozzi D, Verrone GB, Agostini S, Bartolini M, D'Amico G, Pradella S, Miele V. Acute penile trauma: imaging features in the emergency setting. Radiol Med. 2019 Dec;124(12):1270-1280. doi: 10.1007/s11547-019-01065-1. Epub 2019 Jul 13. PMID: 31302847.
2. Hatzimouratidis K, Amar E, Eardley I, Giuliano F, Hatzichristou D, Montorsi F, Vardi Y, Wespes E; European Association of Urology. Guidelines on male sexual dysfunction: erectile dysfunction and premature ejaculation. Eur Urol. 2010 May;57(5):804-14. doi: 10.1016/j.eururo.2010.02.020. Epub 2010 Feb 20. PMID: 20189712.
3. He L, Wen J, Jiang X, Chen H, Tang Y. Long-term efficacy and safety of self-intracavernous injection of prostaglandin E1 for treatment of erectile dysfunction in China. Andrologia. 2011 Jun;43(3):208-12. doi: 10.1111/j.1439-0272.2010.01091.x. Epub 2011 Mar 25. PMID: 21486416.
4. British Association of Urological Surgeons. Penile injection for erection. [Online]. [Accessed 23 August 2020]. Available from http://www.baus.org.uk
5. Moemen MN, Hamed HA, Kamel II, Shamloul RM, Ghanem HM. Clinical and sonographic assessment of the side effects of intracavernous injection of vasoactive substances. Int J Impot Res. 2004 Apr;16(2):143-5. doi: 10.1038/sj.ijir.3901194. PMID: 15014552.
6. Cozzi D, Verrone GB, Agostini S, Bartolini M, D'Amico G, Pradella S, Miele V. Acute penile trauma: imaging features in the emergency setting. Radiol Med. 2019 Dec;124(12):1270-1280. doi: 10.1007/s11547-019-01065-1. Epub 2019 Jul 13. PMID: 31302847.

{kind=link}