Hepatic adenoma with focal hepatocellular carcinoma [Aug 2016]
August 11, 2016CEUS Beyond Europe – Chinese Experience
September 19, 2016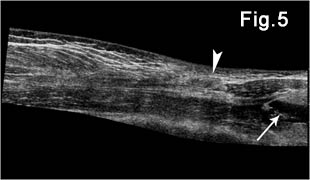
Bilateral quadriceps muscles and suprapatellar recesses injuries: ultrasound evaluation
1. Radiology Department, AHEPA University General Hospital of Thessaloniki, Greece.
2. 2. Radiology Department, "G. GENNIMATAS" General Hospital of Thessaloniki, Greece.
Corresponding author: Vasileios Rafailidis. Radiology Department, AHEPA University Hospital,
Thessaloniki, Greece
Email: billraf@hotmail.com
![Bilateral quadriceps muscles and suprapatellar recesses injuries: ultrasound evaluation [Sep 2016]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotm_sept2016-fig1.jpg)
![Bilateral quadriceps muscles and suprapatellar recesses injuries: ultrasound evaluation [Sep 2016]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotm_sept2016-fig2.jpg)
![Bilateral quadriceps muscles and suprapatellar recesses injuries: ultrasound evaluation [Sep 2016]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotm_sept2016-fig3.jpg)
![Bilateral quadriceps muscles and suprapatellar recesses injuries: ultrasound evaluation [Sep 2016]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotm_sept2016-fig4.jpg)
![Bilateral quadriceps muscles and suprapatellar recesses injuries: ultrasound evaluation [Sep 2016]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotm_sept2016-fig5.jpg)
![Bilateral quadriceps muscles and suprapatellar recesses injuries: ultrasound evaluation [Sep 2016]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotm_sept2016-fig6.jpg)
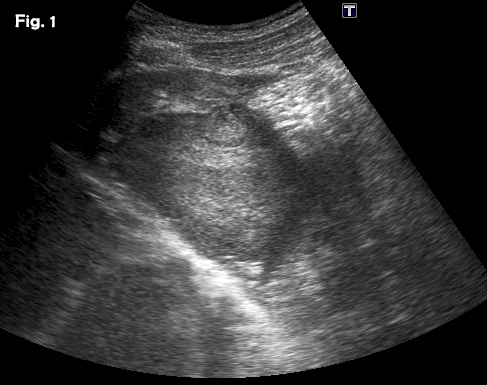
A 49-year-old male patient presented to the emergency department after a heavy object fell on his thighs, causing contusion of both of his quadriceps muscles. Clinical observation revealed linear retraction of the skin on the right suprapatellar area. X-Rays of the femoral bones and knee joints bilaterally didn’t show any fracture. Ultrasound examination revealed contusion of the left vastus medialis muscle and a small amount of fluid in the ipsilateral suprapatellar pouch. (Fig.1,2) The right quadriceps muscle appeared injured at its distal part. There was hyperechogenicity of the right rectus femoris muscle and its fascicular pattern was ill- defined, as a result of the extended contusion of the muscle’s belly. There was also contusion of the right vastus lateralis and intermedius muscles and rupture of intermedius belly peripherally. The subcutaneous tissue appeared hyperechoic and thickened due to edema. (Fig.3) Fluid with a three layer stratification pattern was noted within the right suprapatellar recess. The three layers included an anterior echogenic layer, an anechoic layer in the middle and a hypoechoic layer posteriorly. Fluid also appeared within the lateral and medial bursae of the right knee. (Fig.4, 5) An MRI a few days later confirmed the US findings. (Fig.6)
Direct external muscle trauma may occur in the form of a contusion, haematoma and partial or complete rupture.[1] Contusions affect the actual site of external trauma whereas strains caused by indirect trauma and eccentric contraction typically affect the myotendinous junction.[1,2,3,4] Contusions are graded as mild, moderate or severe depending on the extent of muscle fibers involved and limitation of joint function.[2,5] Undiagnosed or poorly treated muscle lesions can result in long-term complications like cicatricial fibrosis, calcification, fluid collection, serohematic pseudocysts and muscle hernias.[2,4,5] Although clinical examination usually suggests the diagnosis, imaging is imperative in some cases for establishing the final diagnosis.[2] Ultrasonography is the primary imaging modality for the diagnostic work-up of muscle injuries given its advantages, whereas MRI is reserved for some limited cases due to its cost and limited availability. In mild contusion, immediately after injury muscle tissue appears ill-defined hyperechoic due to hemorrhagic infiltration, while perifascial fluid can be seen.[1,2,4,6] In moderate cases, muscle fibers may be ruptured and a haematoma may appear, causing enlargement of the muscle belly. The haematoma may be formed immediately or some days after the contusion and appears anechoic in the acute phase but gradually becomes hyperechoic due to the organization of fibrous tissue. [2,6,7] In severe cases there is complete muscle rupture, resulting in retraction of the belly. The muscle ends can be then seen floating within the haematoma, as in our case. During the healing process, poorly delimited hyperechoic areas are occasionally found and represent scars causing local retraction of muscle fibers.[1,2,6] Dynamic US of the muscle during contraction can be used to better appreciate muscular retraction and make the defect more prominent. Color Doppler technique may identify hyperemia peripherally to the traumatic lesion.[2,4] When it comes to the vastus muscles, the vastus lateralis and intermedialis are usually affected by injuries resulting in partial or complete rupture, because of their exposed location (and their proximity to the femur).[2,4] US demonstrates a discontinuity of the normal striated echogenicity pattern and internal haematomas.[2] MRI can be used in cases of limited visualization of muscle injuries with US, for example in deep injuries. MRI is also considered superior to US for monitoring the muscle healing process.[5,6]
2. Pasta G, Nanni G, Molini L, Bianchi S. Sonography of the quadriceps muscle: Examination technique, normal anatomy, and traumatic lesions. J Ultrasound 2010; 13(2):76–84.
3. Hamilton B, Valle X, Rodas G, Til L, Grive RP, Rincon JA, et al. Classification and grading of muscle injuries: a narrative review. Br J Sports Med 2015 Mar;49(5):306.
4. Lee JC, Healy J. Sonography of lower limb muscle injury. AJR Am J Roentgenol. 2004 Feb;182(2):341-51.
5. Natsis K, Lyrtzis C, Noussios G, Papathanasiou E, Anastasopoulos N, Totlis T. Bilateral rectus femoris intramuscular haematoma following simultaneous quadriceps strain in an athlete: a case report. J Med Case Rep 2010; 4:56.
6. Hayashi D, Hamilton B, Guermazi A, de Villiers R, Crema MD, Roemer FW. Traumatic injuries of thigh and calf muscles in athletes: role and clinical relevance of MR imaging and ultrasound. Insights Imaging. 2012;3(6):591-601.
7. Guillodo Y, Bouttier R, Saraux A. Value of sonography combined with clinical assessment to evaluate muscle injury severity in athletes. J Athl Train 2011;46(5):500-4.
A. Grayscale sonography of the site of trauma revealed partial muscle disruption creating a defect which is filled with a hypoechoic haematoma (arrowhead). There was also an ill-defined hyperechoic area surrounding the muscle fiber disruption, corresponding to edema and hemorrhagic changes (arrow).
B. Power Doppler imaging shows blood flow signals around the injured area.
Figure 2:Longitudinal views of the left-sided thigh
A. Panoramic view of the vastus medialis muscle showing swelling of the distal part of the belly with focal irregularities and changes of the echogenicity pattern (arrow).
B. Longitudinal grayscale image peripherally to Fig. A showing a small quantity of fluid within the left suprapatellar recess (arrow).
Figure 3: Longitudinal B-mode views of the right thigh.
A. Vastus intermedius and rectus femoris contusion. A gap filled with haematoma (thick arrow) is present in the vastus intermedius muscle throughout its width. There are small partial tears of the rectus femoris (arrow) at the site of traumatic skin retraction. Notice the diffuse subcutaneous edema.
B. Gray scale image showing the rupture of the peripheral part of the vastus intermedius with defect, filled with anechoic fluid from local haematoma. The torn muscle fragments are seen freely floating inside the haematoma, a sign referred to as the “bell clapper sign”.
Figure 4: Panoramic Ultrasonography of the distended right suprapatellar recess
A. Longitudinal panoramic view showing an enlarged suprapatellar recess measuring 72 Χ22 Χ 80 mm filled with a layered effusion. A hyperechoic layer is floating over an anechoic layer, which lies on a third layer of low-reflectivity echoes.
B. Transverse panoramic view over the suprapatellar recess with the three layers of echogenicity, over the femoral bone cortex reflection (asterisk).
Figure 5:Fig. 5 Longitudinal panoramic view showing the relation of injured vastus intermedialis and rectus femoris with the suprapatellar recess fluid collection (arrow), the haematoma and diffuse subcutaneous edema (arrowhead). The torn vastus tendon appears proximally retracted.
Figure 6. Confirmation of ultrasound findings with MRI.
Axial (A) and coronal (B) ΜR image of the injured muscles and suprapatellar recesses

{kind=link}