Non Hodgkin lymphoma of the small intestine [Aug 2019]
August 24, 2019Abdominal intracavitary, VUR & HyCoSy
September 26, 2019
One dip too far: an unusual cause of exercise induced chest pain
AUTHORS:
Cillian McNamara1 , Mehul Parekh2, Julia K Prague3, Ian Sinha4, Dimitri Amiras1
1 – Department of Radiology, St. Mary’s Hospital, Imperial College Healthcare NHS Trust
2 – Department of Medicine, St. Mary’s Hospital, Imperial College Healthcare NHS Trust
3 – Department of Endocrinology, St. Mary’s Hospital, Imperial College Healthcare NHS Trust
4 – Department of Orthopaedic Surgery, St. Mary’s Hospital, Imperial College Healthcare NHS Trust
Cillian McNamara1 , Mehul Parekh2, Julia K Prague3, Ian Sinha4, Dimitri Amiras1
1 – Department of Radiology, St. Mary’s Hospital, Imperial College Healthcare NHS Trust
2 – Department of Medicine, St. Mary’s Hospital, Imperial College Healthcare NHS Trust
3 – Department of Endocrinology, St. Mary’s Hospital, Imperial College Healthcare NHS Trust
4 – Department of Orthopaedic Surgery, St. Mary’s Hospital, Imperial College Healthcare NHS Trust
![One dip too far: an unusual cause of exercise induced chest pain </br> [Sep 2019]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/COTM-Sept2019Figure1ARROW.png)
![One dip too far: an unusual cause of exercise induced chest pain </br> [Sep 2019]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/COTM-September2019Figure-2.jpg)
![One dip too far: an unusual cause of exercise induced chest pain </br> [Sep 2019]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/COTM-September2019Figure3ARROW.png)
![One dip too far: an unusual cause of exercise induced chest pain </br> [Sep 2019]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/COTM-September2019Figure4ARROW.png)
![One dip too far: an unusual cause of exercise induced chest pain </br> [Sep 2019]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/COTM-September2019Figure5ARROW.png)
1Clinical History
A 28-year-old radiology registrar experienced sudden onset chest pain while performing tricep dip exercises on holidays. Following the acute injury, the central chest pain was persistent and was exacerbated by breathing and coughing. In the 6 months prior to injury he had been experiencing excessive tiredness, polydipsia and polyuria. Past medical history only included mild asthma. On examination there was exquisite tenderness on palpation of the sternum, just below the level of the sternomanubrial joint. Bloods revealed elevated calcium of 2.77mmol/L (2.2-2.6mmol/L) and an inappropriately elevated parathyroid hormone of 11.7pmol/L (1.6-7.2 pmol/L). Vitamin D level was normal at 82.7nmol/L (70-150nmol/L). HbA1c was 33mmol/mol, and a biochemical screen for additional secondary causes of osteoporosis was otherwise negative.
2Image Findings
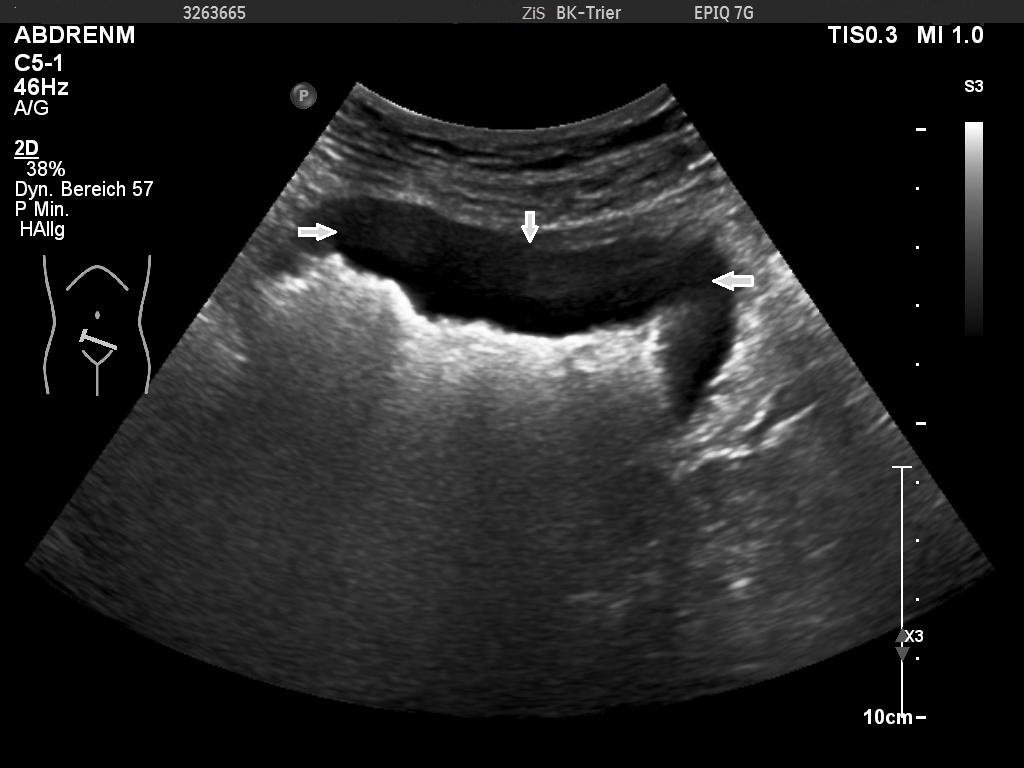
An ultrasound examination of the chest performed using a Toshiba Aplio 500 high-frequency probe showed an acute linear fracture through the anterior cortex of the sternum just below the level of the sternomanubrial joint (FIGURE 1). The subjacent third costal cartilage was unremarkable. A bone densitometry DEXA scan showed osteoporosis of the L2-L4 vertebral bodies with both T-score and Z-scores measuring -2.9 (FIGURE 2). Bone density of the bilateral femora was normal (T score -0.9). Further imaging of the neck was arranged to investigate the cause of the inappropriate parathyroid hormone levels. An ultrasound of the neck revealed a well-defined, hypoechoic nodule located just inferior to the lower pole of the left lobe of the thyroid gland measuring 14x8x5mm (FIGURE 3). The patient then underwent a SPECT-CT of the neck and chest to ensure co-localisation on two imaging modalities. 739 MBq of technetium 99m was injected and acquisitions were obtained at 10min, 90mins and 180mins following tracer injection. Analysis of the SPECT data demonstrated a well-defined area of retained activity situated in the lower pole of the left lobe of the thyroid which correlated well with the findings of the ultrasound scan (FIGURE 4). The overall appearances were in keeping with a parathyroid adenoma situated in the lower pole of the left lobe of the thyroid. The CT component of the study also showed a further view of the fracture (FIGURE 5).
3Diagnosis
Acute sternal fracture secondary to primary hyperparathyroidism resulting from a parathyroid adenoma.
4Discussion
Background:
Sternal fractures are most commonly associated with blunt anterior chest trauma and are widely reported in the medical literature . Sternal insufficiency fractures in patients with osteoporosis are reported although these more commonly occur in elderly patients. Insufficiency fractures occur when normal mechanical stresses are repeatedly applied across abnormal bone, most commonly secondary to osteoporosis. During chest wall exercises, upper body stresses are transmitted to the sternum through the pectoral muscles, costal cartilages and clavicles meaning repetitions of such exercises can lead to sternal injury when the underlying bone is abnormal . Similar cases have previously been reported in military recruits who were performing repetitive tricep dips during their induction training . Sternal fractures can be difficult to diagnose clinically as they are often mistaken for muscle strains or sternoclavicular joint disorders. In the emergent setting, sternal fractures have been investigated as possible acute coronary syndromes given the differential diagnosis when presenting with chest pain in the setting of exercise . Primary hyperparathyroidism is characterised by an inappropriately elevated level of parathyroid hormone (PTH). It is typically caused by a single, benign parathyroid adenoma in 80% of cases but can also be secondary to multiglandular adenomas such as in multiple endocrine neoplasia type 1, parathyroid gland hyperplasia, or rarely a parathyroid carcinoma. On imaging, a parathyroid adenoma is usually seen as a well-defined homogenous, hypoechoic and hypervascualar nodule which may or may not contain cystic regions. Adenomas are perithyroidal in over 90% of cases and can be ectopic in location in 5-10% with the carotid sheath, mediastinum, great vessels or cardiac border being the locations involved given the embryology origins of the glands. US is most useful in identifying adenomas located close to the thyroid gland or the cervical portion of the thymus. 99mTc-sestamibi sctintigraphy can be used to either confirm the location of the adenoma visualised on US scanning or locate ectopic adenomas. This nuclear medicine study is based on the preferential uptake of sestamibi in mitochondria-rich parathyroid adenoma cells.
Clinical perspective:
Atraumatic, low impact fractures warrant further clinical review and investigation as they may be the first presentation of sequelae of secondary causes of reduced bone mineral density that require treatment. This is particularly the case in young adults.
Therapy planning:
For patients with an identified single parathyroid adenoma and end-organ complications such as osteoporosis and/or renal stones treatment is with a minimally invasive parathyroidectomy of the one affected gland. This is particularly the case in young patients. Intra-operative measurement of PTH is often helpful.
Outcome:
The aim of parathyroidectomy of the affected gland is complete cure, which is defined as the reestablishment of normal calcium homeostasis lasting for at least 6 months. In patients with sporadic primary hyperparathyroidism complete cure is achieved in 95% of patients following surgery.
Prognosis:
Bone mineral density improves considerably following parathyroidectomy and normalisation of calcium homeostasis. It is appropriate to repeat assessment of bone densitometry 18 months post-operatively.
Sternal fractures are most commonly associated with blunt anterior chest trauma and are widely reported in the medical literature . Sternal insufficiency fractures in patients with osteoporosis are reported although these more commonly occur in elderly patients. Insufficiency fractures occur when normal mechanical stresses are repeatedly applied across abnormal bone, most commonly secondary to osteoporosis. During chest wall exercises, upper body stresses are transmitted to the sternum through the pectoral muscles, costal cartilages and clavicles meaning repetitions of such exercises can lead to sternal injury when the underlying bone is abnormal . Similar cases have previously been reported in military recruits who were performing repetitive tricep dips during their induction training . Sternal fractures can be difficult to diagnose clinically as they are often mistaken for muscle strains or sternoclavicular joint disorders. In the emergent setting, sternal fractures have been investigated as possible acute coronary syndromes given the differential diagnosis when presenting with chest pain in the setting of exercise . Primary hyperparathyroidism is characterised by an inappropriately elevated level of parathyroid hormone (PTH). It is typically caused by a single, benign parathyroid adenoma in 80% of cases but can also be secondary to multiglandular adenomas such as in multiple endocrine neoplasia type 1, parathyroid gland hyperplasia, or rarely a parathyroid carcinoma. On imaging, a parathyroid adenoma is usually seen as a well-defined homogenous, hypoechoic and hypervascualar nodule which may or may not contain cystic regions. Adenomas are perithyroidal in over 90% of cases and can be ectopic in location in 5-10% with the carotid sheath, mediastinum, great vessels or cardiac border being the locations involved given the embryology origins of the glands. US is most useful in identifying adenomas located close to the thyroid gland or the cervical portion of the thymus. 99mTc-sestamibi sctintigraphy can be used to either confirm the location of the adenoma visualised on US scanning or locate ectopic adenomas. This nuclear medicine study is based on the preferential uptake of sestamibi in mitochondria-rich parathyroid adenoma cells.
Clinical perspective:
Atraumatic, low impact fractures warrant further clinical review and investigation as they may be the first presentation of sequelae of secondary causes of reduced bone mineral density that require treatment. This is particularly the case in young adults.
Therapy planning:
For patients with an identified single parathyroid adenoma and end-organ complications such as osteoporosis and/or renal stones treatment is with a minimally invasive parathyroidectomy of the one affected gland. This is particularly the case in young patients. Intra-operative measurement of PTH is often helpful.
Outcome:
The aim of parathyroidectomy of the affected gland is complete cure, which is defined as the reestablishment of normal calcium homeostasis lasting for at least 6 months. In patients with sporadic primary hyperparathyroidism complete cure is achieved in 95% of patients following surgery.
Prognosis:
Bone mineral density improves considerably following parathyroidectomy and normalisation of calcium homeostasis. It is appropriate to repeat assessment of bone densitometry 18 months post-operatively.
5Teaching Points
Atraumatic sternal fracture should prompt further clinical review and investigation for underlying causes of low bone density; and particularly in younger patients.
6References
[1.] Brookes JG, Dunn RJ, Rogers IR. Sternal fractures: A retrospective analysis of 272 cases. J Trauma. 1993;35:46–54.
[2.] Baker, J. C., & Demertzis, J. L. (2016). Manubrial stress fractures diagnosed on MRI: report of two cases and review of the literature. Skeletal Radiology, 45(6), 833–837.
[3.] Hill PF, Chatterji S, DeMello WF, Gibbons JRP. Stress fracture of the sternum: an unusual injury? Injury. 1997;28(5–6):359–61.
[4.] Wang DM, Zeng QY, Chen SB, Gong Y, Hou ZD, Xiao ZY. Prevalence and risk factors of osteoporosis in patients with ankylosing spondylitis: a 5-year follow-up study of 504 cases. Clin Exp Rheumatol. 2015;33(4):465–70.
[5.] Khan AA, Hanley DA, Rizzoli R, et al. Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus. Osteoporos Int. 2017;28(1):1–19.
[2.] Baker, J. C., & Demertzis, J. L. (2016). Manubrial stress fractures diagnosed on MRI: report of two cases and review of the literature. Skeletal Radiology, 45(6), 833–837.
[3.] Hill PF, Chatterji S, DeMello WF, Gibbons JRP. Stress fracture of the sternum: an unusual injury? Injury. 1997;28(5–6):359–61.
[4.] Wang DM, Zeng QY, Chen SB, Gong Y, Hou ZD, Xiao ZY. Prevalence and risk factors of osteoporosis in patients with ankylosing spondylitis: a 5-year follow-up study of 504 cases. Clin Exp Rheumatol. 2015;33(4):465–70.
[5.] Khan AA, Hanley DA, Rizzoli R, et al. Primary hyperparathyroidism: review and recommendations on evaluation, diagnosis, and management. A Canadian and international consensus. Osteoporos Int. 2017;28(1):1–19.

{kind=link}