Multiparametric ultrasound and AI of Papillary Carcinoma [Oct 2022]
December 30, 2022
Ultrasound diagnosis of bladder endometriosis [Dec 2022]
February 20, 2023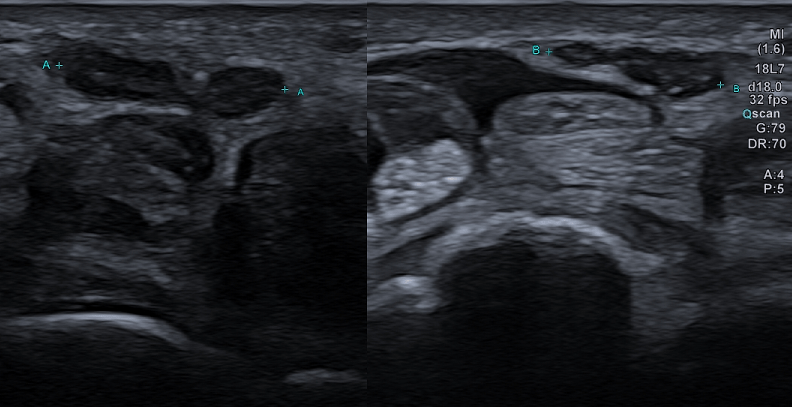
Bifid median nerve with persistent median artery in carpal tunnel syndrome: assessment with US
AUTHORS
Mar Perez-Peña
Carmen Alonso
Cecilia Quispe
Radiology Deparment Alvarez-Buylla Hospital, Mieres, Asturias. Spain
*Corresponding author:
Mar Perez-Peña mar_perez@yahoo.com
Mar Perez-Peña
Carmen Alonso
Cecilia Quispe
Radiology Deparment Alvarez-Buylla Hospital, Mieres, Asturias. Spain
*Corresponding author:
Mar Perez-Peña mar_perez@yahoo.com
Video 1: Pulsatile persistent median artery in between the two branches of bifid median nerve
Video 2: Bifurcation of median nerve at the level of carpal tunnel
1Clinical History
53-year-old woman with paresthesia, pain and weakness of the right hand worsened by sleep, which is mitigated by shaking the hand. She also suffers from sensory deficit in the median innervated region of the hand. Electrophysiologic studies depicted malfunction of the median nerve.
2Image findings
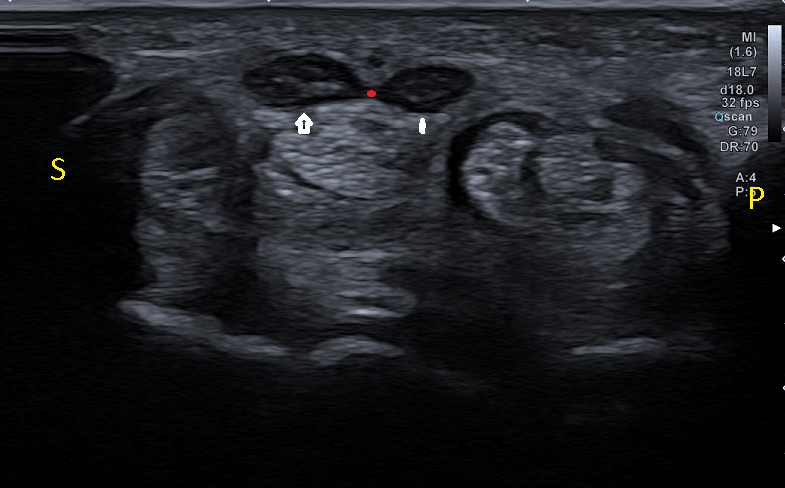
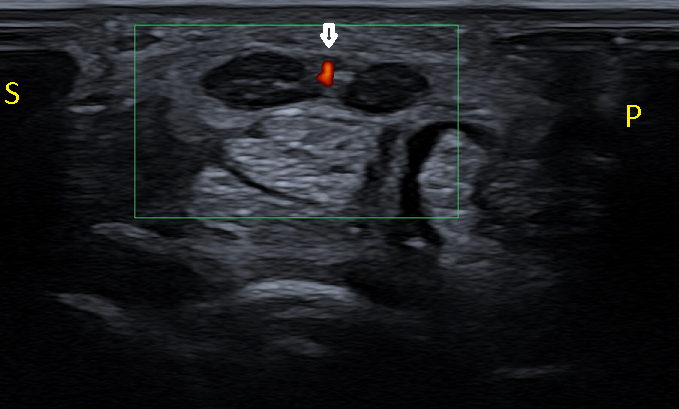
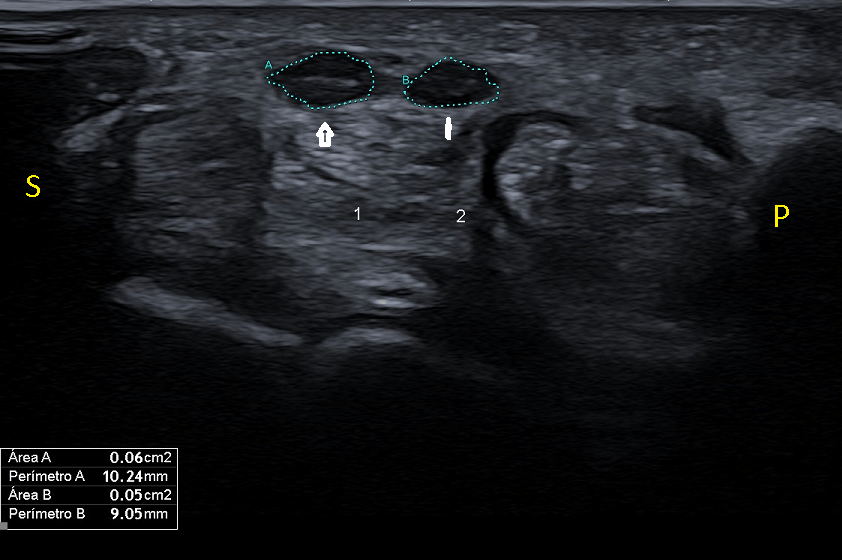
Gray scale ultrasound (US) examination performed on a transverse plane with a 8-14 MHz linear probe shows bifid median nerve with two enlarged nerve trunks joined by a septum underneath the transverse carpal ligament (fig.1). Doppler ultrasound shows vascular pulsatile structure lying anteriorly, in the cleft between the two trunks, consistent with persistent median artery (fig.2). Both, ulnar and radial branches of the bifid nerve are thickened, with an area of 6mm2 for lateral and 5mm2 for medial trunks with a total area of 11mm2 (fig.3), findings consistent with carpal tunnel syndrome.
On the contralateral carpal tunnel there is also a bifid nerve with persistent artery with no signs of enlargement. (fig.4).
Videos 1 and 2 also show the findings described.
3DIAGNOSIS
DISCUSSION
A bifid median nerve is an uncommon anatomical variation in the forearm that it can be accompanied by a persistent median artery with an incidence described in the literature of less than 3%.
Although the median nerve usually divides into two or three branches after exiting the distal edge of transverse carpal ligament, sometimes it may divide in two bundles in the distal forearm and appear as a bifid median nerve in the carpal tunnel. A bifid median nerve may be accompanied by an accessory artery, the persistent median artery of the forearm, which lies in between the two nerve bundles. The artery and bifid nerve can be enclosed by a common epineurium.
Although questioned by authors, bifid median nerve may more commonly develop carpal tunnel syndrome because of its relatively higher global cross sectional area. For bifid median nerve, the size criterion for the diagnosis of carpal tunnel syndrome is slightly higher than for a non-bifid median nerve. Data suggest an optimal cut-off value of 11mm2 for median nerve cross sectional area in bifid nerves.
CLINICAL PERSPECTIVE
The diagnosis of carpal tunnel syndrome is traditionally based on clinical history, physical examination, and electrophysiologic study results, but ultrasonography (US) has revealed to be an accurate and useful diagnostic tool in these patients.
US allows depiction of anatomical variants such as bifid median nerve, as well as other causes of compression of median nerve in the carpal tunnel, such as ganglia, tenosynovitis or tumors in the flexor compartment of the wrist. It also provides measurement of median nerve cross sectional area, that contributes to the diagnosis of this condition.
As shown in this case, bifid median nerves associated with a persistent median artery are important to diagnose for their clinical and surgical implications. The knowledge of the existence of bifid median nerve is important in planning surgical decompression of median nerve to avoid nerve injury or potential relapse if decompression of both branches has not been done. It is also important to diagnose a persistent median artery to prevent its section when performing the surgery.
THERAPY PLANNING:
Surgical decompression by transection of the transverse carpal ligament is the indicated treatment of carpal tunnel syndrome. Currently, endoscopic carpal tunnel release is the treatment of choice, but the risk of median nerve injury increases when anatomic variation is present, because of difficulty in seeing the branches at operation. In the case of a bifid median nerve the two branches may be separately constricted and require separate decompression. For these reasons in cases of bifid median nerve an open carpal tunnel release is preferred by surgeons.
OUTCOME & PROGNOSIS:
The patient had an uneventful postoperative course with almost complete resolution of preoperative symptoms in the postoperative visit. The resolution of symptoms was complete and even the sleep disturbance was solved. She was able to perform regular duties with her hand.
A bifid median nerve is an uncommon anatomical variation in the forearm that it can be accompanied by a persistent median artery with an incidence described in the literature of less than 3%.
Although the median nerve usually divides into two or three branches after exiting the distal edge of transverse carpal ligament, sometimes it may divide in two bundles in the distal forearm and appear as a bifid median nerve in the carpal tunnel. A bifid median nerve may be accompanied by an accessory artery, the persistent median artery of the forearm, which lies in between the two nerve bundles. The artery and bifid nerve can be enclosed by a common epineurium.
Although questioned by authors, bifid median nerve may more commonly develop carpal tunnel syndrome because of its relatively higher global cross sectional area. For bifid median nerve, the size criterion for the diagnosis of carpal tunnel syndrome is slightly higher than for a non-bifid median nerve. Data suggest an optimal cut-off value of 11mm2 for median nerve cross sectional area in bifid nerves.
CLINICAL PERSPECTIVE
The diagnosis of carpal tunnel syndrome is traditionally based on clinical history, physical examination, and electrophysiologic study results, but ultrasonography (US) has revealed to be an accurate and useful diagnostic tool in these patients.
US allows depiction of anatomical variants such as bifid median nerve, as well as other causes of compression of median nerve in the carpal tunnel, such as ganglia, tenosynovitis or tumors in the flexor compartment of the wrist. It also provides measurement of median nerve cross sectional area, that contributes to the diagnosis of this condition.
As shown in this case, bifid median nerves associated with a persistent median artery are important to diagnose for their clinical and surgical implications. The knowledge of the existence of bifid median nerve is important in planning surgical decompression of median nerve to avoid nerve injury or potential relapse if decompression of both branches has not been done. It is also important to diagnose a persistent median artery to prevent its section when performing the surgery.
THERAPY PLANNING:
Surgical decompression by transection of the transverse carpal ligament is the indicated treatment of carpal tunnel syndrome. Currently, endoscopic carpal tunnel release is the treatment of choice, but the risk of median nerve injury increases when anatomic variation is present, because of difficulty in seeing the branches at operation. In the case of a bifid median nerve the two branches may be separately constricted and require separate decompression. For these reasons in cases of bifid median nerve an open carpal tunnel release is preferred by surgeons.
OUTCOME & PROGNOSIS:
The patient had an uneventful postoperative course with almost complete resolution of preoperative symptoms in the postoperative visit. The resolution of symptoms was complete and even the sleep disturbance was solved. She was able to perform regular duties with her hand.
4Teaching Points
1. Ultrasound should be performed preoperatively in carpal tunnel syndrome to reveal morphological variants of the median nerve or other conditions that may compress the nerve in the carpal tunnel.
2. Bifid median nerve with a persistent median artery in the carpal tunnel may be associated with a higher incidence of carpal tunnel syndrome and is very important to diagnose for its clinical and surgical significance.
2. Bifid median nerve with a persistent median artery in the carpal tunnel may be associated with a higher incidence of carpal tunnel syndrome and is very important to diagnose for its clinical and surgical significance.
5Informed consent
I declare that consent from the patient was obtained to publish this case.
6References
1. Klauser AS, Halpern EJ, Faschingbauer R, et al. Bifid median nerve in carpal tunnel syndrome: assessment with US cross-sectional area measurement. Radiology. 2011;259(3):808-15.
2. Propeck T, Quinn TJ, Jacobson JA, Paulino AF, Habra G, Darian VB. Sonography and MR imaging of bifid median nerve with anatomic and histologic correlation. AJR Am J Roentgenol. 2000;175(6):1721-5.
3. Narayan S. Bifid median nerve in a patient with carpal tunnel syndrome: A case report and literature review. Australas J Ultrasound Med. 2016 ;19(4):164-168.
4. Gassner EM, Schocke M, Peer S, Schwabegger A, Jaschke W, Bodner G. Persistent median artery in the carpal tunnel: color Doppler ultrasonographic findings. J Ultrasound Med. 2002 ;21(4):455-61.
5. Chen L, Chen J, Hu B, Jiang LX. Sonographic findings of the bifid median nerve and persistent median artery in carpal tunnel: a preliminary study in chinese individuals. Clinics (Sao Paulo). 2017 ;72(6):358-362.
6. Kostoris F, Bassini S, Longo E, Murena L. Carpal Tunnel Syndrome Associated with Bifid Median Nerve and Palmaris Profundus - Case Report and Literature Review. The Journal of Hand Surgery (Asian-Pacific Volume) 2019;24(2), 238–242.
2. Propeck T, Quinn TJ, Jacobson JA, Paulino AF, Habra G, Darian VB. Sonography and MR imaging of bifid median nerve with anatomic and histologic correlation. AJR Am J Roentgenol. 2000;175(6):1721-5.
3. Narayan S. Bifid median nerve in a patient with carpal tunnel syndrome: A case report and literature review. Australas J Ultrasound Med. 2016 ;19(4):164-168.
4. Gassner EM, Schocke M, Peer S, Schwabegger A, Jaschke W, Bodner G. Persistent median artery in the carpal tunnel: color Doppler ultrasonographic findings. J Ultrasound Med. 2002 ;21(4):455-61.
5. Chen L, Chen J, Hu B, Jiang LX. Sonographic findings of the bifid median nerve and persistent median artery in carpal tunnel: a preliminary study in chinese individuals. Clinics (Sao Paulo). 2017 ;72(6):358-362.
6. Kostoris F, Bassini S, Longo E, Murena L. Carpal Tunnel Syndrome Associated with Bifid Median Nerve and Palmaris Profundus - Case Report and Literature Review. The Journal of Hand Surgery (Asian-Pacific Volume) 2019;24(2), 238–242.

{kind=link}