Pilomatricoma: A Case Report with Pathological Confirmation [Sept 2022]
November 1, 2022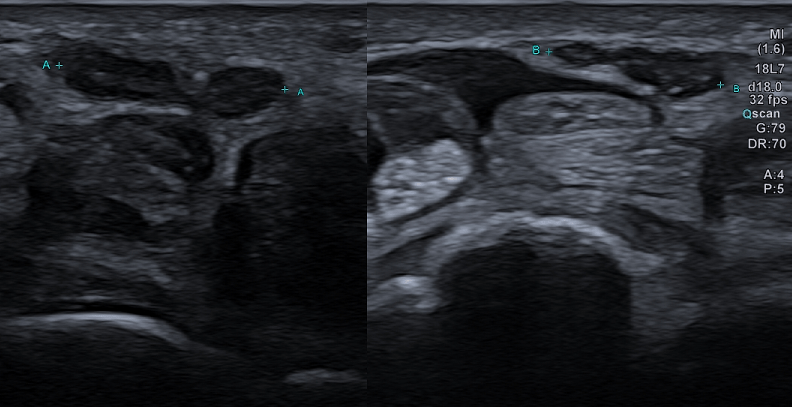
Bifid median nerve with persistent median artery in carpal tunnel syndrome: assessment with US [Nov 2022]
January 12, 2023
Multiparametric ultrasound and AI of Papillary Carcinoma
AUTHORS
Chiara Di Bella [1],
Carmen Solito [1],
Vincenzo Dolcetti [1],
Giuseppe Tiziano Lucarelli [1],
Vito Cantisani [1] [1] Policlinico Umberto I, Dipartimento di Scienze Radiologiche, Università La Sapienza, Rome, Italy
*Corresponding author:
Chiara Di Bella
Policlinico Umberto I, Dipartimento di Scienze Radiologiche, Università La Sapienza, Rome, Italy
Email: chiaradibella@uniroma1.it
Chiara Di Bella [1],
Carmen Solito [1],
Vincenzo Dolcetti [1],
Giuseppe Tiziano Lucarelli [1],
Vito Cantisani [1] [1] Policlinico Umberto I, Dipartimento di Scienze Radiologiche, Università La Sapienza, Rome, Italy
*Corresponding author:
Chiara Di Bella
Policlinico Umberto I, Dipartimento di Scienze Radiologiche, Università La Sapienza, Rome, Italy
Email: chiaradibella@uniroma1.it
1Clinical History
A 34-year-old patient was admitted to our hospital because of thyroid function indices alteration. She denied trauma, infection, and had no positive family history disease of neck’s region.
The clinical examination did not show any significant signs.
2Image findings
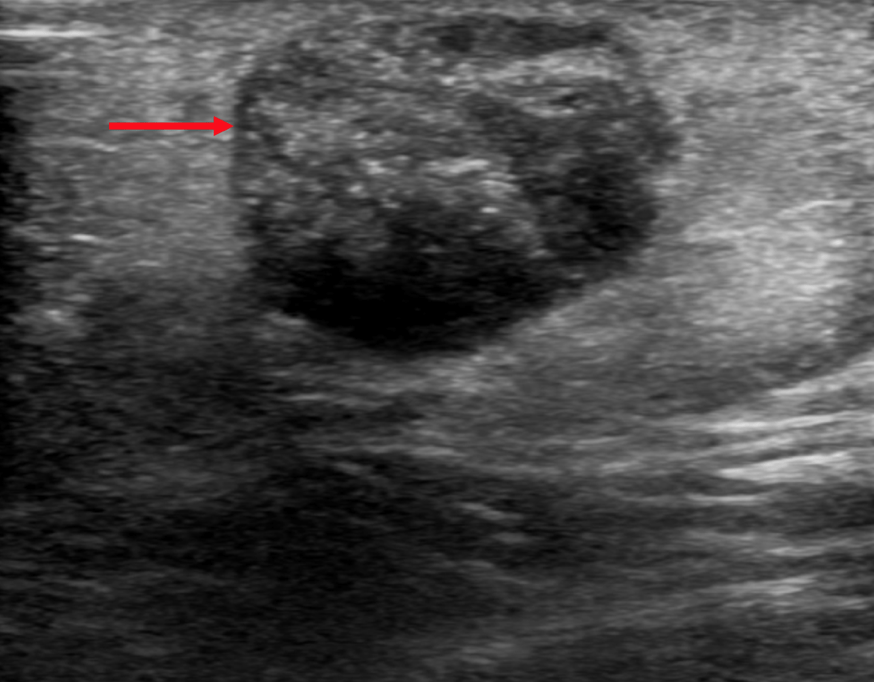
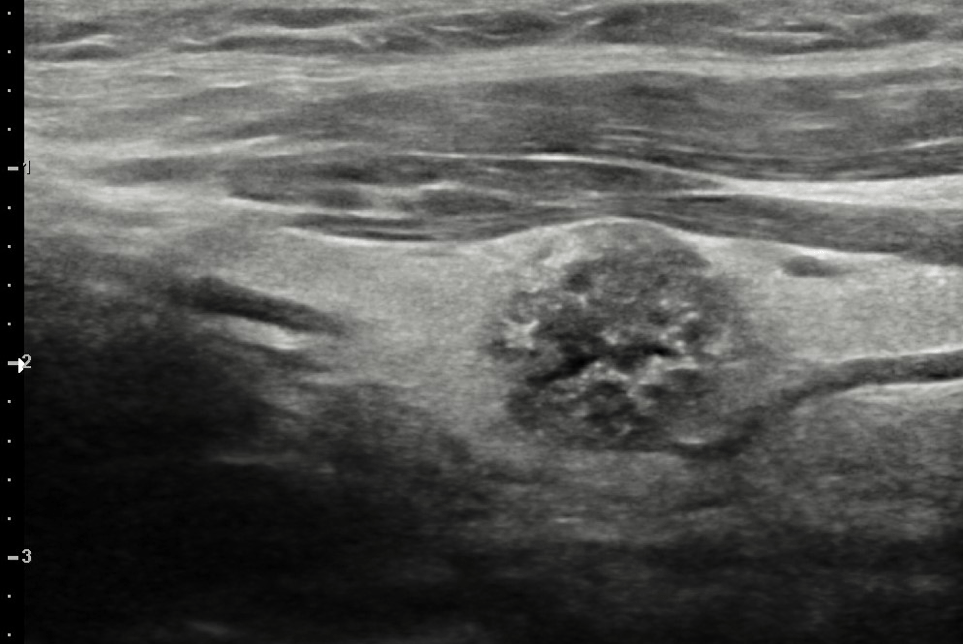
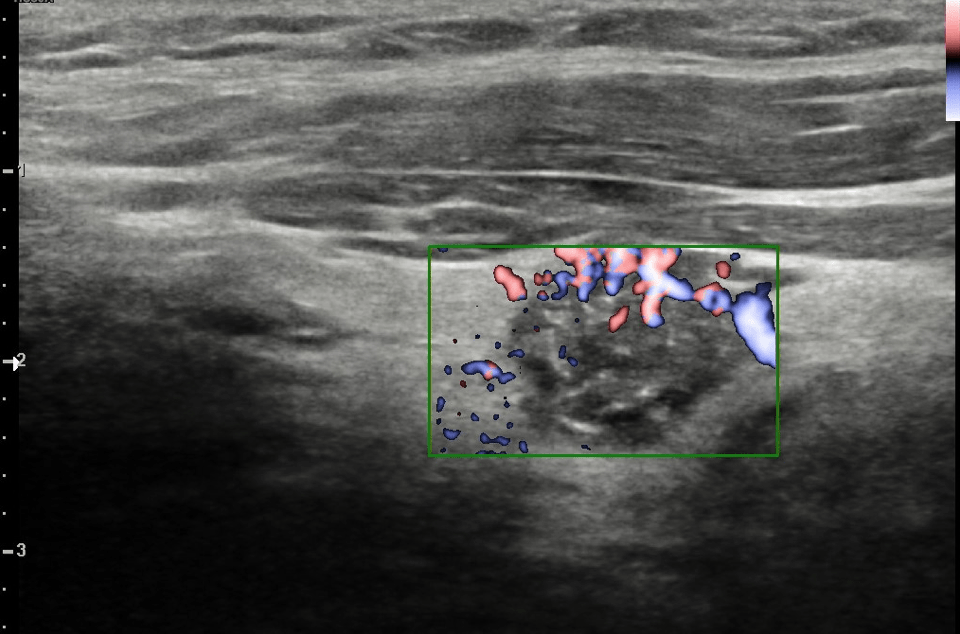
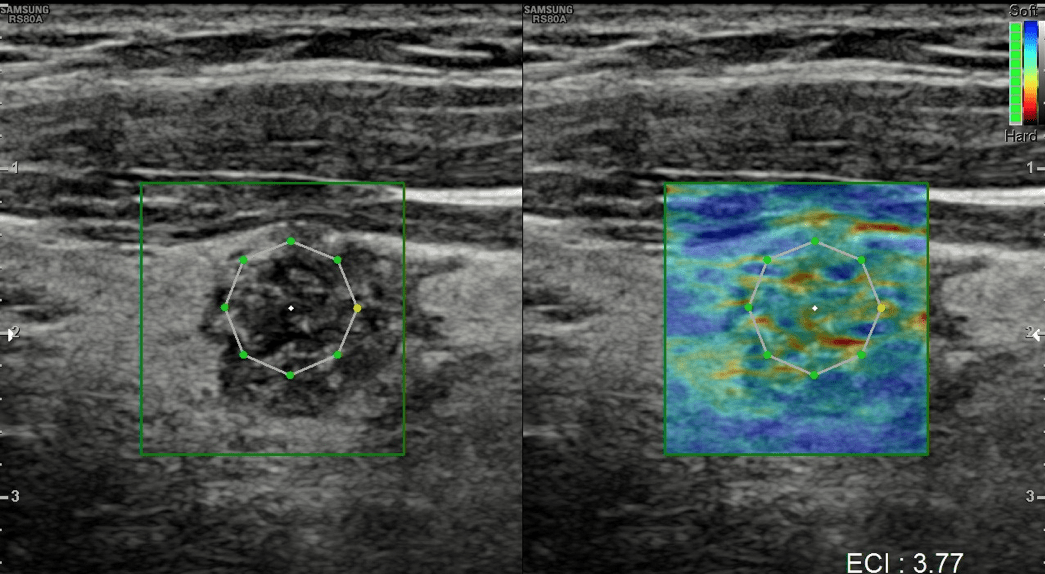
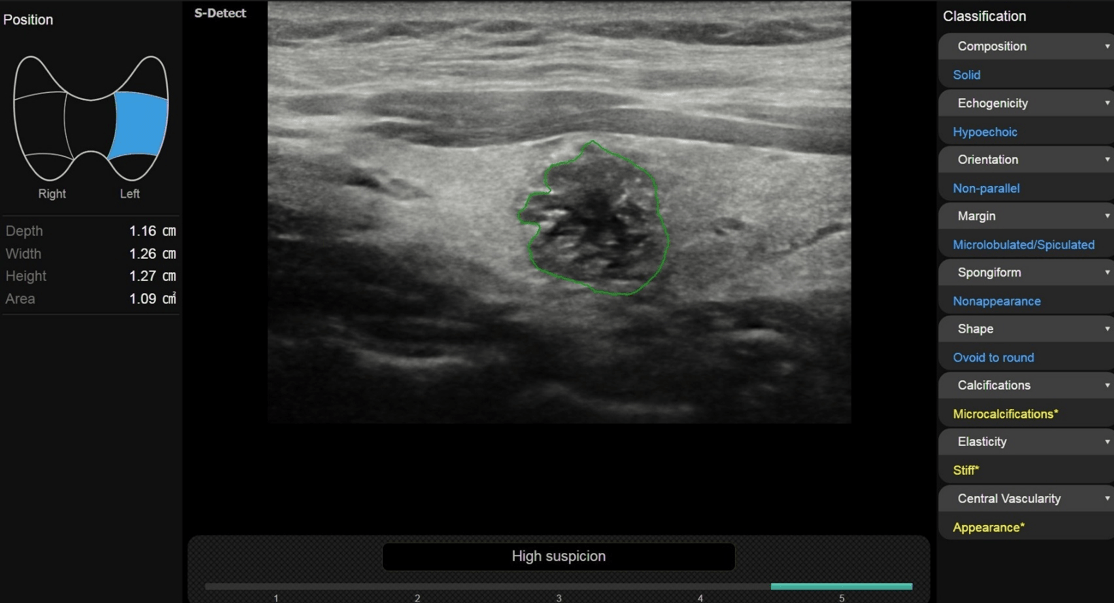
Gray scale ultrasound (US) examination showed the thyroid in situ and volumetrically within limits. It showed inhomogeneous echostructure due to the presence of thin hyperechoic striae referable to fibrosclerotic phenomena and at least two nodular lesions, the largest one located in the left lobe, with hypoechoic ecostructure, irregular margins, internal microcalcifications (Fig.1), in addition, the color-power-Doppler evaluation reported increased parenchymal vascularization and peri and intranodular vascularization patterns (Fig.2); the lesion also appaeared stiff at US-elastosonography (USE) with elasticity contrast index (ECI): 3.77 (Fig.3). AI S-Detect software classified it as TIRADS 5 (Fig.4).
Some lymph nodes of increased size, with short subcentimetric axis, at the level of the VI station, however with non-specific and not easily distinguishable compared to lymph nodes reactive to chronic thyroiditis
Some lymph nodes of increased size, with short subcentimetric axis, at the level of the VI station, however with non-specific and not easily distinguishable compared to lymph nodes reactive to chronic thyroiditis
3Diagnosis
Excisional biopsy was performed and the histopathological examination was consistent with multifocal classic variant papillary thyroid carcinoma.
4Discussion
BACKGROUND
Papillary carcinoma accounts for 80-90% of all thyroid cancers. It can be familiar in up to 5% of patients. In some patients, the tumor is multifocal and can affect both lobes of the thyroid gland. The tumor extends lymphatically to the regional lymph nodes in 1/3 of the patients and can give lung metastases. Papillary carcinoma often develop in between 30 and 60 years old., with a female predominance (F:M = 3:1).
CLINICAL PERSPECTIVE
Papillary carcinoma is almost always asymptomatic although in more advanced forms there may be clinical signs due to compression or infiltration such as dysphonia, dysphagia or dyspnea.
THERAPY PLANNING:
Tumours > 4 cm or widely infiltrating require a total or almost total thyroidectomy, with post-surgical ablation of the residual thyroid tissue by radioiodine, administered when the patient is hypothyroid or after injection of thyroid stimulating hormone (TSH) recombinant.
After this treatment, suppressive levothyroxine of TSHe is administered. Treatment of capsulated tumors < 4 cm localized in a single lobe is usually almost-total thyroidectomy, although some specialists recommend surgical treatment of lobectomy and istmectomy.
OUTCOME & PROGNOSIS:
Surgical treatment is almost always decisive. TSH is administered at suppressive doses in order to minimize the risk of recurrence and to cause regression of any microscopic residue of papillary carcinoma.
Papillary carcinoma accounts for 80-90% of all thyroid cancers. It can be familiar in up to 5% of patients. In some patients, the tumor is multifocal and can affect both lobes of the thyroid gland. The tumor extends lymphatically to the regional lymph nodes in 1/3 of the patients and can give lung metastases. Papillary carcinoma often develop in between 30 and 60 years old., with a female predominance (F:M = 3:1).
CLINICAL PERSPECTIVE
Papillary carcinoma is almost always asymptomatic although in more advanced forms there may be clinical signs due to compression or infiltration such as dysphonia, dysphagia or dyspnea.
THERAPY PLANNING:
Tumours > 4 cm or widely infiltrating require a total or almost total thyroidectomy, with post-surgical ablation of the residual thyroid tissue by radioiodine, administered when the patient is hypothyroid or after injection of thyroid stimulating hormone (TSH) recombinant.
After this treatment, suppressive levothyroxine of TSHe is administered. Treatment of capsulated tumors < 4 cm localized in a single lobe is usually almost-total thyroidectomy, although some specialists recommend surgical treatment of lobectomy and istmectomy.
OUTCOME & PROGNOSIS:
Surgical treatment is almost always decisive. TSH is administered at suppressive doses in order to minimize the risk of recurrence and to cause regression of any microscopic residue of papillary carcinoma.
5Teaching Points
TIRADS is one of the main resources for the radiological characterization of the thyroid nodule, however its accuracy is variable because it is mainly based on the gray scale and therefore may not be sufficiently specific or sensitive for diagnosis as there are several suspicious features of malignancy that may not be present in the lesion for analysis. To overcome this limit, USE is assuming an increasingly important role due to its ability to assess the hardness of the thyroid nodule, which is an important sign of malignancy (1). The USE is a technique of thyroid elastography that uses the pulsation of the carotid artery as a source of internal pulsation, so as to reduce the limits of elastography, such as the variability that could be caused by different levels of compression by the operators (2). This method has the advantage that no free-hand external compression is used and therefore is less operator-dependent. It is both qualitative (color coded elastograms) and semiquantitative with strain ratio computations. The operator holds the probe over the thyroid applying no pressure and the anteroposterior displacement of thyroid tissue caused by the carotid pulsation is followed with a motion tracking technique and used to calculated the strain images (elastograms) (3). From a practical point of view, elastography is performed by placing the probe on the thyroid without applying compression, the patient is asked to briefly hold his breath and the operator expects the sidebar to turn green. After manually creating a ROI containing the injury (but not containing the carotid artery), the ECI is automatically calculated.
A further valuable help can be provided by the use of computer-assisted diagnosis (CAD) systems, such as S-Detect which analyzes the characteristics of nodular thyroid formation contained within the ROI and classifies them according to TIRADS. This software is integrated in sonographic equipment and help in the detection and evaluation of thyroid nodules by using the various subset of ML approaches that uses neural networks arranged in layers to extract higher level features from input data and automatically learn their discriminative features, which allows approximation of non-linear relationships with excellent performance (4).
To conclude the ultrasound finding of a "taller-than-wide" hypoechoic nodular formation with irregular or shaded contours and presence of hyperechoic spots caused by microcalcifications (psammoma bodies) must induce the suspicion of carcinomatous papillary lesion, especially if present in a non-thyroid goitre. In the diagnosis is precious the help of the color-power-doppler that shows peripheral spots or rich intranodular vascularization with anarchist distribution; the use of CAD systems and the detection of an ECI > 3 contribute to a diagnosis of malignant injury.
A further valuable help can be provided by the use of computer-assisted diagnosis (CAD) systems, such as S-Detect which analyzes the characteristics of nodular thyroid formation contained within the ROI and classifies them according to TIRADS. This software is integrated in sonographic equipment and help in the detection and evaluation of thyroid nodules by using the various subset of ML approaches that uses neural networks arranged in layers to extract higher level features from input data and automatically learn their discriminative features, which allows approximation of non-linear relationships with excellent performance (4).
To conclude the ultrasound finding of a "taller-than-wide" hypoechoic nodular formation with irregular or shaded contours and presence of hyperechoic spots caused by microcalcifications (psammoma bodies) must induce the suspicion of carcinomatous papillary lesion, especially if present in a non-thyroid goitre. In the diagnosis is precious the help of the color-power-doppler that shows peripheral spots or rich intranodular vascularization with anarchist distribution; the use of CAD systems and the detection of an ECI > 3 contribute to a diagnosis of malignant injury.
6Conflicts of Interest
The authors have no competing interests to declare that are relevant to the content of this case report.
7References
1. Fresilli D, David E, Pacini P, et al.. Thyroid nodule characterization: how to assess the malignancy risk. Update of the literature. Diagnostics (Basel). 2021;11(8):1374.
2. Hahn SY, Shin JH, Ko EY, Bae JM, Choi JS, Park KW. Complementary role of elastography using carotid artery pulsation in the ultrasonographic assessment of thyroid nodules: a prospective study. Korean J Radiol. 2018 ;19(5):992-999.
3. Cantisani V, Grazhdani H, Drakonaki E, et al. . Strain US elastography for the characterization of thyroid nodules: advantages and limitation. Int J Endocrinol. 2015; 2015: 908575.
4. Sorrenti S, Dolcetti V, Radzina M, et al.. Artificial Intelligence for thyroid nodule characterization: where are we standing? Cancers (Basel). 2022;14(14):3357.
2. Hahn SY, Shin JH, Ko EY, Bae JM, Choi JS, Park KW. Complementary role of elastography using carotid artery pulsation in the ultrasonographic assessment of thyroid nodules: a prospective study. Korean J Radiol. 2018 ;19(5):992-999.
3. Cantisani V, Grazhdani H, Drakonaki E, et al. . Strain US elastography for the characterization of thyroid nodules: advantages and limitation. Int J Endocrinol. 2015; 2015: 908575.
4. Sorrenti S, Dolcetti V, Radzina M, et al.. Artificial Intelligence for thyroid nodule characterization: where are we standing? Cancers (Basel). 2022;14(14):3357.

{kind=link}