Ultrasound findings in Sars-Cov2-Infection of the lung [August 2021]
July 30, 2021
The role of ultrasound in detection and characterisation of incidental Renal Cell Carcinomas [October 2021]
September 30, 2021
Diagnosing Thoracic Aortic Dissection using Bedside Ultrasound in an Emergency Department in a Norwegian University Teaching Hospital
AUTHORS
Jay Chotai M.D., Department of Emergency Medicine, Department of Haematology, Akershus Universitetssykehus
Tone Dolva Dahl M.D., Ph.D., Department of Internal Medicine, Akershus Universitetssykehus
Irida Vavecka, M.D., Department of Cardiology, Akershus Universitetssykehus
Jay Chotai M.D., Department of Emergency Medicine, Department of Haematology, Akershus Universitetssykehus
Tone Dolva Dahl M.D., Ph.D., Department of Internal Medicine, Akershus Universitetssykehus
Irida Vavecka, M.D., Department of Cardiology, Akershus Universitetssykehus
1Abstract
Thoracic aortic dissection (TAD) is a medical emergency which can present with a variety of symptoms. It is vital to rapidly identify and diagnose this condition to increase the patients’ survival chances. Computed tomography (CT), and Magnetic resonant imaging (MRI) are the standard diagnostic modalities, however these are normally carried out outside an emergency department which could delay diagnosis and delivery of care.
Transthoracic Echocardiography (TTE) is an accepted first line imaging modality in an Emergency department. This has been previously reported by the European Association of Echocardiography[1], and ultrasound is becoming widely available and used in Emergency Departments nowadays.
The aim of this article is to present a case in which bedside ultrasound with focused cardiac examination (FOCUS) was utilised to provide a rapid diagnosis of a clinical suspected aortic dissection.
The aim of this article is to present a case in which bedside ultrasound with focused cardiac examination (FOCUS) was utilised to provide a rapid diagnosis of a clinical suspected aortic dissection.
2Case
a 55-year-old male was admitted to the emergency department at Akershus University Teaching hospital, Norway. He complained of chest pain radiating to the left jaw, with concomitant visual disturbances to his left eye. He was a former smoker and had a history of asthma and borderline hypertension.
On admission, the patient had no complaints except for mild pain in his left jaw and chest as described previously as well as normal vision. The physical examination showed a significant blood pressure difference in the upper extremities; 135/85 mmHg on the left arm and 100/70 mmHg on right arm. Other vital signs were unremarkable. He had a strong holosystolic cardiac murmur, which was not previously known. There were no palpable masses in the abdomen, and the neurological examination was normal.
ECG showed no signs of acute ischemia. His lab test showed a hemoglobin of 15.4 g/dL, CRP 3 mg/L, ALAT 65 U/L, creatinine 104 µmol/L, troponin T 9 ng/L, NT-proBNP 67 ng/L and lactate 3.1 mmol/L.
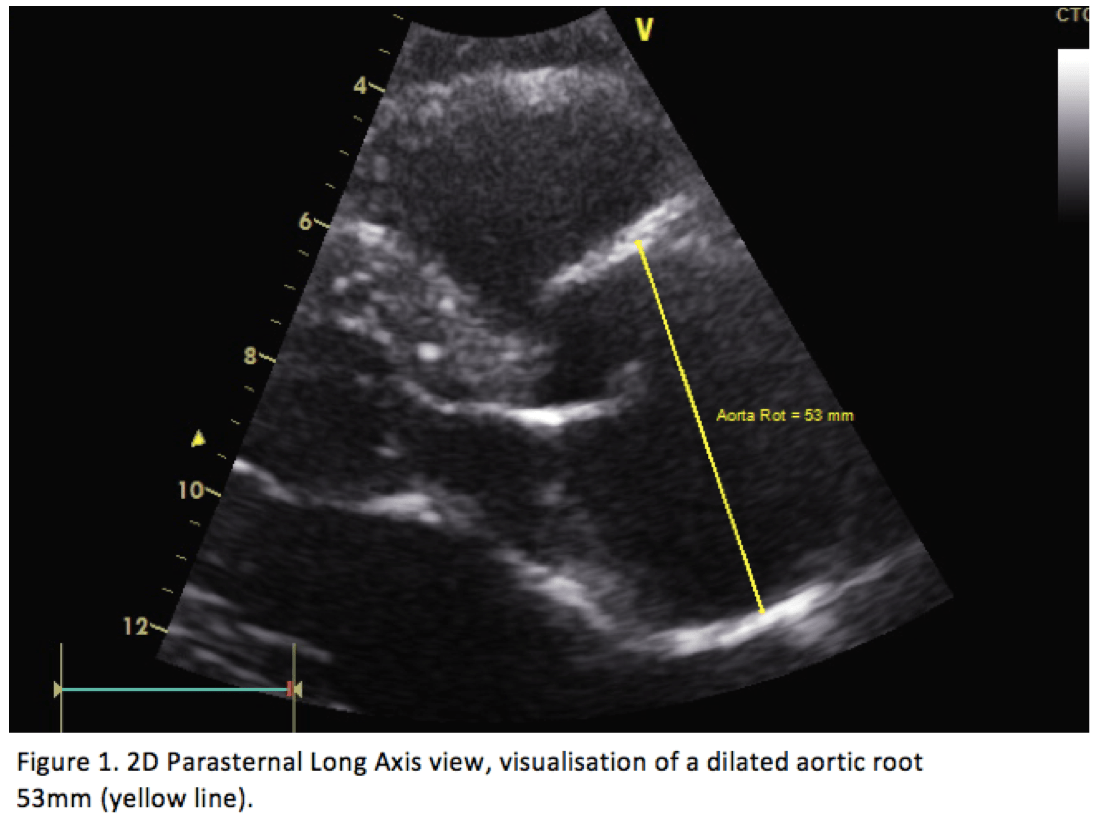
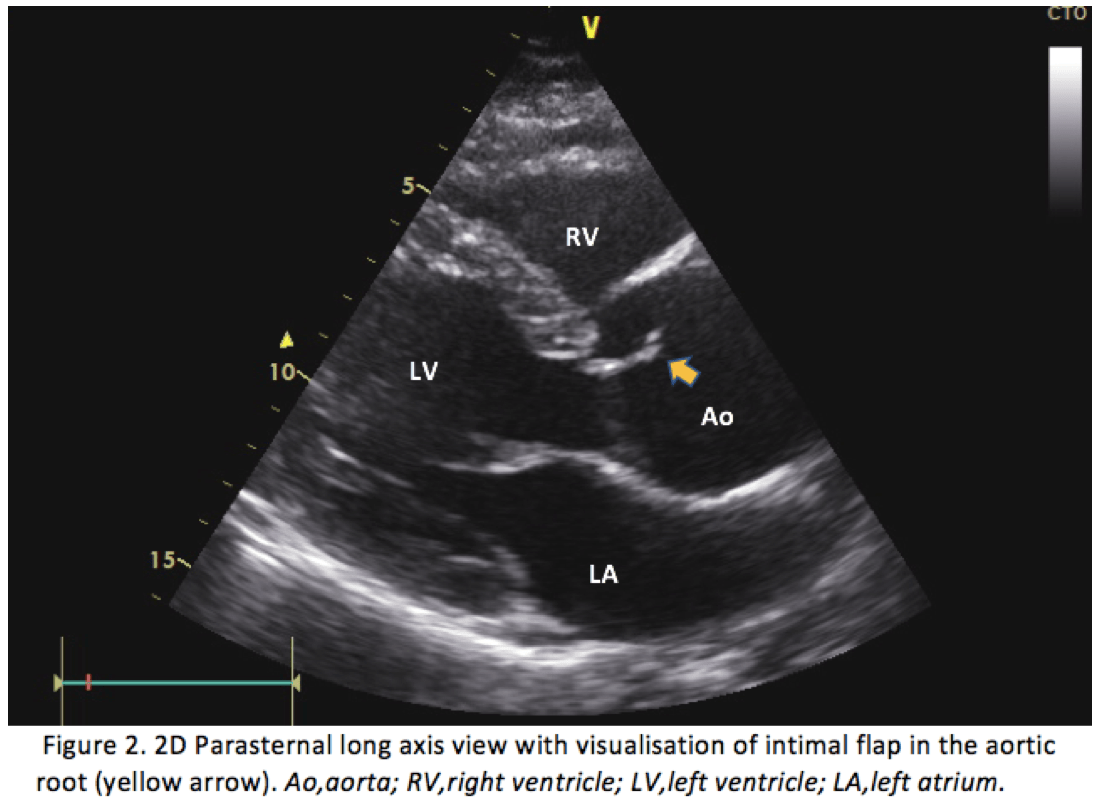
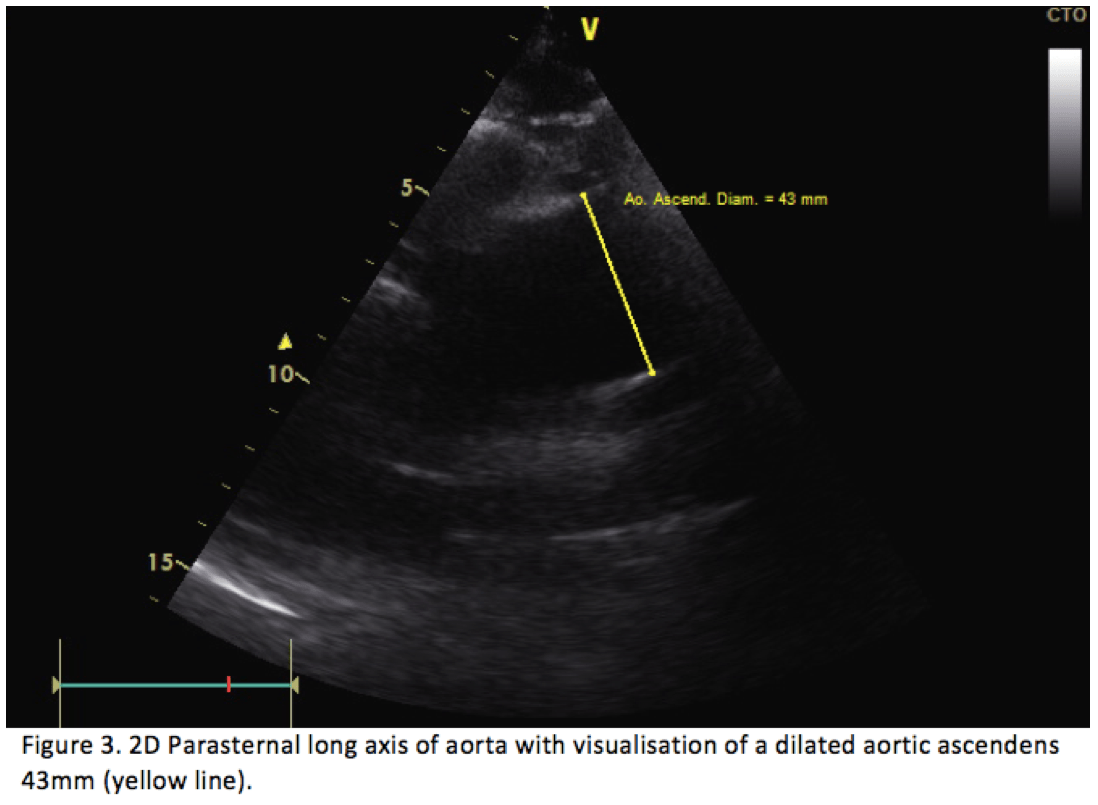
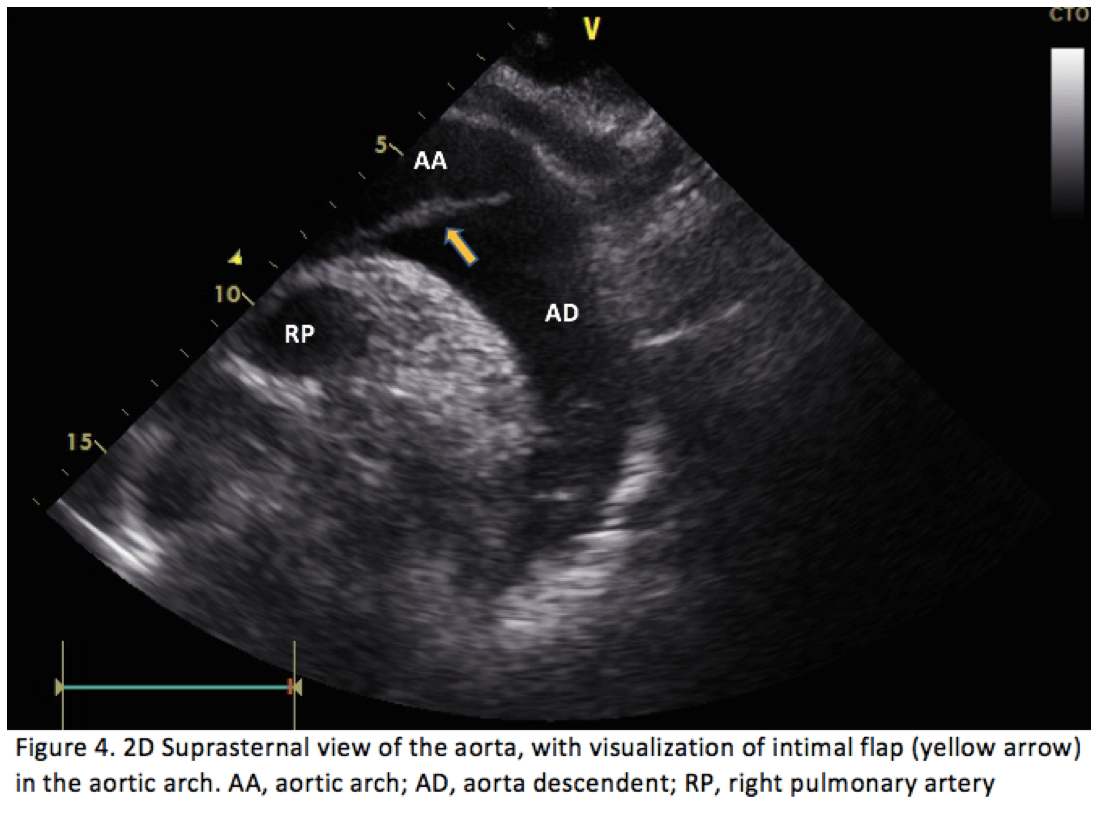
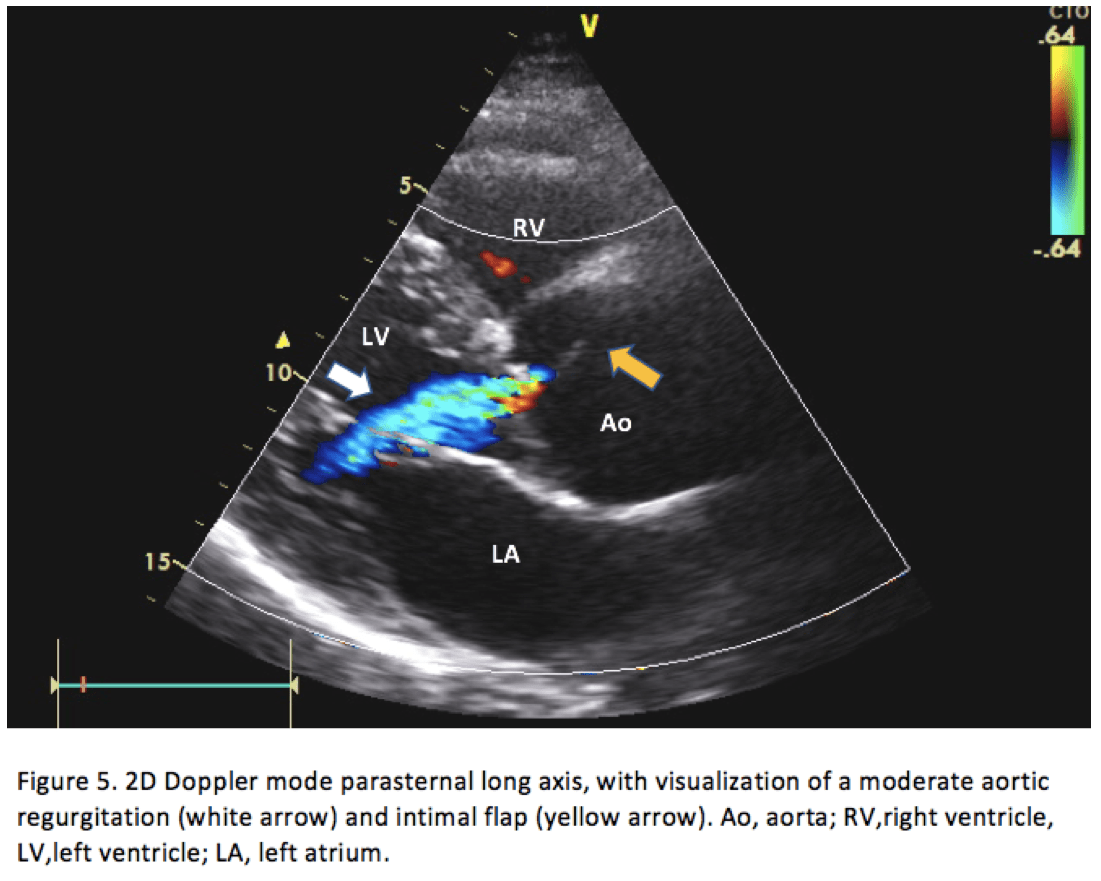
Bedside FOCUS study revealed a dilated aortic root of 53 mm (Figure 1.) and a proximal ascending aorta of 43 mm (Figure 3). The parasternal long axis projection and suprasternal projection, showed an intimal flap in the aortic arch and ascending aorta extending down to the aortic valve. This can be visualized in Figures 2,4 & 5 below. There was moderate aortic regurgitation (Figure 5), which was presumed secondary to the aortic dissection. There was no pericardial effusion, and the abdominal aorta was not examined.
A CT was also requested which confirmed a Stanford type A Aortic Dissection from the aortic valve to below the renal arteries. The patient was transferred to the thoracic surgery facility at Oslo University Hospital and underwent urgent surgery.
On admission, the patient had no complaints except for mild pain in his left jaw and chest as described previously as well as normal vision. The physical examination showed a significant blood pressure difference in the upper extremities; 135/85 mmHg on the left arm and 100/70 mmHg on right arm. Other vital signs were unremarkable. He had a strong holosystolic cardiac murmur, which was not previously known. There were no palpable masses in the abdomen, and the neurological examination was normal.
ECG showed no signs of acute ischemia. His lab test showed a hemoglobin of 15.4 g/dL, CRP 3 mg/L, ALAT 65 U/L, creatinine 104 µmol/L, troponin T 9 ng/L, NT-proBNP 67 ng/L and lactate 3.1 mmol/L.
Bedside FOCUS study revealed a dilated aortic root of 53 mm (Figure 1.) and a proximal ascending aorta of 43 mm (Figure 3). The parasternal long axis projection and suprasternal projection, showed an intimal flap in the aortic arch and ascending aorta extending down to the aortic valve. This can be visualized in Figures 2,4 & 5 below. There was moderate aortic regurgitation (Figure 5), which was presumed secondary to the aortic dissection. There was no pericardial effusion, and the abdominal aorta was not examined.
A CT was also requested which confirmed a Stanford type A Aortic Dissection from the aortic valve to below the renal arteries. The patient was transferred to the thoracic surgery facility at Oslo University Hospital and underwent urgent surgery.
3Discussion
Thoracic Aortic Dissection (TAD) is a rare condition, with high mortality if untreated. The estimated incidence is 5-10 cases per million, and of the most common underlying medical condition is hypertension[2]. The symptoms and signs of TAD can be seen with other critical medical conditions and is very variable in presentation. Chest pain is present in up to 90% of patients upon admission[3].
Survival rates are increased with early diagnosis, especially when the dissection involves the aortic root which can cause a secondary myocardial infarction or aortic valve failure[4]. The mortality rate is as high as 1% per hour in the first 48 hours without the provision of the necessary treatment[4]. It is deemed important for clinicians to maintain a high level of suspicion to detect the diagnosis and provide treatment as early as possible.
CT and MRI are current standard diagnostic modalities which have largely replaced aortography[5].
Nowadays TTE is widely accessible to emergency physicians, and a focused examination of the heart is a part of ultrasound performance protocols utilised bedside in different settings in emergency departments. Standard imaging of a focus cardiac ultrasound examination (FOCUS) usually includes parasternal long axis, parasternal short axis, and apical view of the heart. The sensitivity and specificity for ultrasound for detection of aortic dissection has been shown to be high in selected studies[6], but the true sensitivity and specificity is probably variable depending on the level of experience of the operator performing the examination[7]. Two echocardiographic features are strongly suggestive of thoracic aortic dissection namely visualization of dilatation of any segment of the aorta and visualisation of an intimal flap in the aorta[8]. FOCUS taken in combination with clinical risk factors for diagnosing aortic dissection also results in higher sensitivities and specificities [9].
4Conclusion
Bedside FOCUS study can be performed by emergency physicians as a screening tool in patients with suspected thoracic aortic dissection. The examination can be performed in a very short space of time, rendering it a very efficient modality of choice for well-trained emergency physicians. This will ensure a more accurate diagnosis and facilitate appropriate aortic imaging and urgent surgical evaluation as indicated. An intimal flap within the aorta and aortic segment dilatation has good sensitivity and specificity for the diagnosis of thoracic aortic dissection. It is important to note that FOCUS should not be used as a standalone test to rule in or rule out thoracic aortic dissection.
5References
1. Evangelista A, Flachskampf FA, Erbel R, Antonini-Canterin F, Vlachopoulos C, Rocchi G, Sicari R, Nihoyannopoulos P, Zamorano J; European Association of Echocardiography; Document Reviewers:, Pepi M, Breithardt OA, Plonska-Gosciniak E. Echocardiography in aortic diseases: EAE recommendations for clinical practice. Eur J Echocardiogr. 2010 Sep;11(8):645-58. doi: 10.1093/ejechocard/jeq056. Erratum in: Eur J Echocardiogr. 2011 Aug;12(8):642. PMID: 20823280.
2. Paul R Sullivan, Allan B Wolfson, Ronald D Leckey, Jane L Burke, Diagnosis of acute thoracic aortic dissection in the emergency department, The American Journal of Emergency Medicine, Volume 18, Issue 1,2000,Pages 46-50,ISSN 0735-6757, https://doi.org/10.1016/S0735-6757(00)90047-0.
3. Strayer RJ, Shearer PL, Hermann LK. Screening, evaluation, and early management of acute aortic dissection in the ED. Curr Cardiol Rev. 2012 May;8(2):152-7. doi: 10.2174/157340312801784970. PMID: 22708909; PMCID: PMC3406274.
4. Blaivas M, Sierzenski PR. Dissection of the proximal thoracic aorta: a new ultrasonographic sign in the subxiphoid view. Am J Emerg Med. 2002 Jul;20(4):344-8. doi: 10.1053/ajem.2002.33006. PMID: 12098184.
5. Williams J, Heiner JD, Perreault MD, McArthur TJ. Aortic dissection diagnosed by ultrasound. West J Emerg Med. 2010;11(1):98-99.
6. Victor MF, Mintz GS, Kotler MN, et al: Two dimensional echocardiographic diagnosis of aortic dissection. Am J Cardiol 1981;48:1155
7. Fojtik JP, Costantino TG, Dean AJ. The diagnosis of aortic dissection by emergency medicine ultrasound. J Emerg Med. 2007 Feb;32(2):191-6. doi: 10.1016/j.jemermed.2006.07.020. Epub 2007 Jan 22. PMID: 17307632.
8. Roudaut RP, Billes MA, Gosse P, et al: Accuracy of M-mode and two-dimensional echocardiography in the diagnosis ofaortic dissection: An experience with 128 cases. Clin Cardiol 1988;11:553- 562
9. Nazerian P, Vanni S, Castelli M, Morello F, Tozzetti C, Zagli G, Giannazzo G, Vergara R, Grifoni S. Diagnostic performance of emergency transthoracic focus cardiac ultrasound in suspected acute type A aortic dissection. Intern Emerg Med. 2014 Sep;9(6):665-70. doi: 10.1007/s11739-014-1080-9. Epub 2014 May 29. PMID: 24871637.
2. Paul R Sullivan, Allan B Wolfson, Ronald D Leckey, Jane L Burke, Diagnosis of acute thoracic aortic dissection in the emergency department, The American Journal of Emergency Medicine, Volume 18, Issue 1,2000,Pages 46-50,ISSN 0735-6757, https://doi.org/10.1016/S0735-6757(00)90047-0.
3. Strayer RJ, Shearer PL, Hermann LK. Screening, evaluation, and early management of acute aortic dissection in the ED. Curr Cardiol Rev. 2012 May;8(2):152-7. doi: 10.2174/157340312801784970. PMID: 22708909; PMCID: PMC3406274.
4. Blaivas M, Sierzenski PR. Dissection of the proximal thoracic aorta: a new ultrasonographic sign in the subxiphoid view. Am J Emerg Med. 2002 Jul;20(4):344-8. doi: 10.1053/ajem.2002.33006. PMID: 12098184.
5. Williams J, Heiner JD, Perreault MD, McArthur TJ. Aortic dissection diagnosed by ultrasound. West J Emerg Med. 2010;11(1):98-99.
6. Victor MF, Mintz GS, Kotler MN, et al: Two dimensional echocardiographic diagnosis of aortic dissection. Am J Cardiol 1981;48:1155
7. Fojtik JP, Costantino TG, Dean AJ. The diagnosis of aortic dissection by emergency medicine ultrasound. J Emerg Med. 2007 Feb;32(2):191-6. doi: 10.1016/j.jemermed.2006.07.020. Epub 2007 Jan 22. PMID: 17307632.
8. Roudaut RP, Billes MA, Gosse P, et al: Accuracy of M-mode and two-dimensional echocardiography in the diagnosis ofaortic dissection: An experience with 128 cases. Clin Cardiol 1988;11:553- 562
9. Nazerian P, Vanni S, Castelli M, Morello F, Tozzetti C, Zagli G, Giannazzo G, Vergara R, Grifoni S. Diagnostic performance of emergency transthoracic focus cardiac ultrasound in suspected acute type A aortic dissection. Intern Emerg Med. 2014 Sep;9(6):665-70. doi: 10.1007/s11739-014-1080-9. Epub 2014 May 29. PMID: 24871637.

{kind=link}