
Merkel cell carcinoma [Jun 2017]
June 11, 2017
Gastric GIST coexisting with primary lung adenocarcinoma [Aug 2017]
August 11, 2017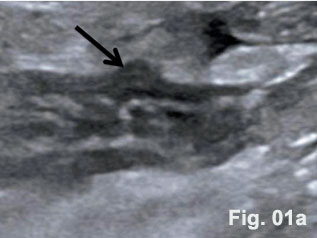
Diverticula and diverticulitis of the appendix
1Medical Department,
2Radiological Department,
3Pathological Department of the Dietrich-Bonhoeffer-Hospital Neubrandenburg.
4Medizinische Klinik 2, Caritas-Krankenhaus Bad Mergentheim
![Diverticula and diverticulitis of the appendix</br> [Jul 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotmjuly2017-fig1a.jpg)
![Diverticula and diverticulitis of the appendix</br> [Jul 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotmjuly2017-fig1b.jpg)
![Diverticula and diverticulitis of the appendix</br> [Jul 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotmjuly2017-fig2.jpg)
![Diverticula and diverticulitis of the appendix</br> [Jul 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotmjuly2017-fig3a.jpg)
![Diverticula and diverticulitis of the appendix</br> [Jul 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/cotmjuly2017-fig3b.jpg)
A 34-year-old complained about a sudden onset of right-lower-quadrant pain. Preoperative ultrasound revealed the appendix with a hypoechoic and thickened wall and the so-called dome sign [Figure 1]. Abdominal tenderness and other clinical signs were suggestive of acute appendicitis. On clinical examination tachycardia (108/min), febrile temperature (38.60 C) and dehydration were documented. Blood test results showed leucocytosis (13,2/nl). Emergency laparoscopic appendecectomy was performed. A large inflammatory mass was found involving the appendix [Figure 2]. The histological specimen revealed the combined presentation of congenital and acquired diverticula. Histopathological examination confirmed phlegmonous inflammation of the appendix and periappendicitis caused by inflammation of diverticula [Figure 3].
Here we present the sonographic findings of a diverticulitis of the appendix including histology. The diverticulum could be clearly displayed in an otherwise thickened appendix with well preserved layers. Diverticula of the appendix can be true or congenital or false (due to acquired mechanisms) [Table 1 and 2] [(1)]. The wall of congenital diverticula contains all the normal histological components of the appendiceal wall. The walls of the acquired or false appendiceal diverticulum are only composed of mucosa, some loose areolar tissue and the serosa. This group either develops during the growth of the fetus or before inflammatory changes make there appearence in the appendix. The prevalence of congenital diverticula found in appendicectomy specimens range from 0,004 % to 0,6 % [(2)]. Diverticulitis of diverticula of the appendix is even rarer. Approximately 78% of cases were associated with varying signs and degrees of inflammation at time of their removal [(3)]. Perforation was observed in 66 % of cases with a high mortality (30-fold compared with acute appendicitis). Four subtypes of appendicular diverticulosis have been described in the literature [Table 2] [(1)]. The majority of diverticula of the appendix described in the literature were incidental findings observed during routine X ray examination of the gastrointestinal tract. While it is agreed that many people with appendiceal diverticula live healthy, normal lives, there can be no doubt that with the onset of complications, life is threatened by inflammation and complications.
| Diverticula | Acquired | Congenital |
| Synonym | True diverticula | Pseudodiverticula |
| Frequency | 3% | 97 % |
| Prevalence (Incidence) | 0,014 % | 1,4 % |
| Age (median) | 31 | 38 |
| Solitary / multiple | Solitary | Multiple or solitary |
| Localisation | Antimesenteric border | Mesenteric or antimesenteric border |
| Type | Diverticulum | Appendix | Description |
| Type 1 | Inflamed | Normal | Normal-appearing appendix with an acutely inflamed diverticulum |
| Type 2 | Inflamed | Inflamed | Acutely inflamed diverticulum with surrounding appendicitis |
| Type 3 | Normal | Inflamed | Conventional appendicitis with an incidental uninvolved diverticulum |
| Type 4 | Normal | Normal | incidental appendiceal diverticulum with no appendicitis |
2. Friedlich M, Malik N, Lecompte M, Ayroud Y. Diverticulitis of the appendix. Can J Surg 2004;47:146-147.
3. Collins DC. Diverticula of the Vermiform Appendix: A Study Based on Thirty Cases. Ann Surg 1936;104:1001-1012.
4. Lange J, Bachmann R, Konigsrainer A, Zdichavsky M. Appendiceal diverticulitis shortly after a performed laparoscopic sigma resection. J Surg Case Rep 2015;2015.
5. Kelynack T N. A contribution to the pathology of the vermiform appendix. London: HK Lewis, 1893.
6. Yacoe ME, Jeffrey RB, Jr. Sonography of appendicitis and diverticulitis. Radiol Clin North Am 1994;32:899-912.
7. Townsend RR, Jeffrey RB, Jr., Laing FC. Cecal diverticulitis differentiated from appendicitis using graded-compression sonography. AJR Am J Roentgenol 1989;152:1229-1230.
8. Dietrich CF, Lembcke B, Jenssen C, Hocke M, Ignee A, Hollerweger A. Intestinal ultrasound in rare gastrointestinal diseases, update, part 1. Ultraschall Med 2014;35:400-421.
9. Dietrich CF, Lembcke B, Jenssen C, Hocke M, Ignee A, Hollerweger A. Intestinal Ultrasound in Rare Gastrointestinal Diseases, Update, Part 2. Ultraschall Med 2015;36:428-456.
10. Nylund K, Maconi G, Hollerweger A, Ripolles T, Pallotta N, Higginson A, Serra C, et al. EFSUMB Recommendations and Guidelines for Gastrointestinal Ultrasound - Part 1: Examination Techniques and Normal Findings (Long version). Ultraschall Med 2016.
11. Nylund K, Maconi G, Hollerweger A, Ripolles T, Pallotta N, Higginson A, Serra C, et al. EFSUMB Recommendations and Guidelines for Gastrointestinal Ultrasound - Part 1: Examination Techniques and Normal Findings (Short version). Ultraschall Med 2016.
12. Lin CH, Chen TC. Diverticulosis of the appendix with diverticulitis: case report. Chang Gung Med J 2000;23:711-715.
13. Kori T, Nemoto M, Maeda M, Tsuzuki Y, Ando T, Sekihara M, Uchida N, et al. Sonographic features of acute colonic diverticulitis: the "dome sign". J Clin Ultrasound 2000;28:340-346.
14. Fitzer PM, Rao KG, Bundrick TJ. Diverticulosis of the appendix: radiographic and clinical features. South Med J 1985;78:1512-1514.
15. Skaane P, Strom EH. Peridiverticulitis of the appendix: an unusual ultrasonic "target lesion". J Clin Gastroenterol 1990;12:353-356.
16. Ripolles T, Martinez-Perez MJ, Morote V, Solaz J. Diseases that simulate acute appendicitis on ultrasound. Br J Radiol 1998;71:94-98.
17. Iki K, Echigo M, Nogami A, Iwamoto S, Takeo T, Tsunoda T, Eto T. Preoperative diagnosis of acute appendiceal diverticulitis by ultrasonography. Surgery 2001;130:87-89.
18. Kubota T, Omori T, Yamamoto J, Nagai M, Tamaki S, Sasaki K. Sonographic findings of acute appendiceal diverticulitis. World J Gastroenterol 2006;12:4104-4105.
19. Kabiri H, Clarke LE, Tzarnas CD. Appendiceal diverticulitis. Am Surg 2006;72:221-223.
20. Yamauchi M, Miyamoto M, Takeuchi K, Fukuhara T. Sonographic appearance of appendiceal diverticulitis. Intern Med 2008;47:1153-1154.
21. Ma KW, Chia NH, Yeung HW, Cheung MT. If not appendicitis, then what else can it be? A retrospective review of 1492 appendectomies. Hong Kong Med J 2010;16:12-17.
22. Nguyen-Tang T, Shah JN, Sanchez-Yague A, Binmoeller KF. Use of the front-view forward-array echoendoscope to evaluate right colonic subepithelial lesions. Gastrointest Endosc 2010;72:606-610.
23. Lourenco RB, Pinho Mda C, Schraibman V, Macedo AL, Francisco Neto MJ, Funari MB. Perforated diverticulitis of the appendix: ultrasonographic diagnosis. Einstein (Sao Paulo) 2011;9:75-77.
24. Willems S, Vanhulle A, Deruyter L. Appendiceal diverticulitis: a rare cause of right iliac fossa pain syndrome. Acta Chir Belg 2011;111:332-334.
25. Osada H, Ohno H, Saiga K, Watanabe W, Okada T, Honda N. Appendiceal diverticulitis: multidetector CT features. Jpn J Radiol 2012;30:242-248.
26. Yamana I, Kawamoto S, Inada K, Nagao S, Yoshida T, Yamashita Y. Clinical characteristics of 12 cases of appendiceal diverticulitis: a comparison with 378 cases of acute appendicitis. Surg Today 2012;42:363-367.
27. Patil AY, Levine MS, Grujic E, Goren RA. Clinical and CT findings in appendiceal diverticulitis. Clin Imaging 2014;38:350-352.
28. Ito D, Miki K, Seiichiro S, Hata S, Kobayashi K, Teruya M, Kaminishi M. Clinical and computed tomography findings of appendiceal diverticulitis vs acute appendicitis. World J Gastroenterol 2015;21:3921-3927.
29. Subramanian M, Chawla A, Chokkappan K, Liu H. Diverticulitis of the appendix, a distinctive entity: preoperative diagnosis by computed tomography. Emerg Radiol 2015;22:609-612.
Figure 2: Surgical Specimen. Diverticula present at the tip and middle third of the appendix along the mesenteric and antimesenteric borders, partly inflamed without perforation. Wall thickening of appendix was more prominent than that seen in typical appendicitis.
Figure 3:Histologic examination of the appendix: Transversal section of the appendix mid with a diverticulum devoid of a distinct Muscularis propria suggestive of an acquired diverticulum (a) and longitudinal section of the appendix tip with a diverticulum consisting parts of the Muscularis propria suggestive of a congenital diverticulum (b).

{kind=link}