Endometriosis infiltrating the sigmoid colon [May 2017]
May 11, 2017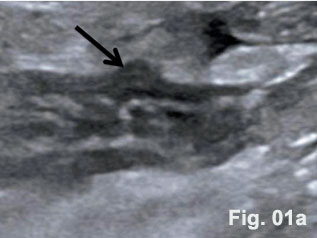
Diverticula and diverticulitis of the appendix [Jul 2017]
July 11, 2017
Merkel cell carcinoma - value of colour-Doppler sonography in the locoregional assessment of tumor spread
M. Staiano: Department of Pathology, National Cancer Institute, Pascale Foundation, via M.Semmola, Naples, I-80131, Italy.
Corresponding Author:
Orlando Catalano, MD, National Cancer Institute, Pascale Foundation, via M.Semmola, Naples, I-80131, Italy.
0039-81-5903664 o.catalano@istitutotumori.na.it
![Merkel cell carcinoma</br> [Jun 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/june2017-1-scaled.jpg)
![Merkel cell carcinoma</br> [Jun 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/june2017-2a.jpg)
![Merkel cell carcinoma</br> [Jun 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/june2017-2b.jpg)
![Merkel cell carcinoma</br> [Jun 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/june2017-3a.jpg)
![Merkel cell carcinoma</br> [Jun 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/june2017-3b.jpg)
![Merkel cell carcinoma</br> [Jun 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/june2017-4a.jpg)
![Merkel cell carcinoma</br> [Jun 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/june2017-4b.jpg)
![Merkel cell carcinoma</br> [Jun 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/june2017-5a.jpg)
![Merkel cell carcinoma</br> [Jun 2017]](http://s834315022.websitehome.co.uk/wp-content/uploads/2020/11/june2017-5b.jpg)
A 68-year-old man came to our observation for a rapidly growing, painless nodule of the postero-lateral aspect of the left thigh, immediately below the buttock. The lesion had developed about six months before but it had initially been diagnosed as a hemangioma, without any investigation. At inspection the lesion was dome-shaped, reddish, and elastic. At sonography imaging the lesion appeared as hypoechoic, with a superficial layer moderately hypoechoic and a deeper layer more markedly hypoechoic. The lesion involved the dermis and the subcutaneous tissue. Maximum diameter was 41 mm and maximum thickness was 29 mm. The margins were ill-defined. At directional power-Doppler imaging there was an intense vascularization, with chaotic but mostly vertical arteries. Spectral Doppler analysis identified a slow velocity, low resistive index profile.
The left inguinal region was investigated, to rule out any regional lymph-node metastasis. In the groin we could find an enlarged lymph-node, measuring 34x14 mm. This lymph-node exhibit a focal hypoechoic nodule in the cortex, which measured 20x11 mm. At power-Doppler imaging this tumor deposit had an intense and anarchic vascularization. A sonography-guided fine-needle aspiration (FNA) of the focal nodule was carried out. Cytology and immunocytology evaluation allowed to diagnose a lymph-node metastasis from Merkel cell carcinoma (MCC).
The patient underwent staging with whole-body, contrast-enhanced computed tomography (CT). CT confirmed the thigh lesion and the lymph-node metastasis but allowed to rule out any distant metastasis. The patient underwent successfully surgery, with wide excision of the primary thigh tumor and with left groin radical lymphadenectomy. The patient is now free of recurrence at two years from surgery.
MCC is a rare but aggressive neuroendocrine tumor of the dermis. Most MCCs develop in the sun-exposed areas of the head and neck or of the extremities. Mean patient age at diagnosis is around 70 years and there is a moderate prevalence of males. The number of MCC is increasing.
MCC tends to be overlooked by the patient in the early stage. However, given its high rate of lymph-node and distant metastasis, a prompt diagnosis and staging would be fundamental to improve survival. MCC is staged as: T1 <2 cm maximum tumor dimension, T2 2-5 cm maximum tumor dimension, T3 >5 cm maximum tumor dimension, T4 primary tumor invades bone, muscle, fascia, or cartilage.
At sonography MCC appears as a hypoechoic, heterogeneous, oval or dome-shaped lesion of the dermis. The overlying echoic epidermis line can be thickened. The lesion has ill-defined margins and the subcutaneous layer is quickly involved by tumor growth. At Doppler imaging MCC is hypervascular, with multiple arteries disposed chaotically inside the tumor. Differential diagnosis includes non-pigmented melanoma, squamous cell carcinoma, cutaneous metastasis, and cutaneous lymphoma.
Excision of the primary tumor represents the treatment of choice. Regional lymph-nodes sonography and sonography-guided FNA or a sentinel lymph-node excision biopsy procedure is performed for the N staging parameter and whole body CT or PET-CT is employed to detect distant metastases.
- Hernández-Aragüés I, Vázquez-Osorio I, Alfageme F, et al. Skin ultrasound features of Merkel cell carcinoma. J Eur Acad Dermatol Venereol 2017 Jan 3. doi: 10.1111/jdv.14102.
- Peloschek P, Novotny C, Mueller-Mang C, et al. Diagnostic imaging in Merkel cell carcinoma: Lessons to learn from 16 cases with correlation of sonography, CT, MRI and PET. Eur J Radiol 2010;73:317-23.
- Righi A, Asioli S, Caliendo V, et al. An ultrasonography-cytology protocol for the diagnostic management of regional nodes in a subset of patients with Merkel cell carcinoma of the skin. Br J Dermatol 2013;168:563-70.
figure 1. Reddish cutaneous nodule of the left thigh (some sonography gel above).
figure 2. Sonography of the thigh showing an ill-defined, bi-layered lesion of the dermis and subdermis (a) with power-Doppler demonstrating hypervascularity (b).
figure 3. Sonography of the groin showing an enlarged lymph-node with a focal, oval tumor deposit (a), appearing hypervascular at power-Doppler imaging (b).
figure 4. Cytology (Papanicolaou coloration) and immunocytology (CD56 marker) of the inguinal lymph-node showing MCC metastasis. figure 5. Contrast-enhanced CT scans showing left inguinal region lymph-node metastasis (a, arrow) and left thigh cutaneous nodule (b).

{kind=link}