An Eye for an Eye [Jan 2023]
April 17, 2023
Student Image Challenge 94
August 29, 2023
SUBMIT YOUR CASE
EFSUMB invites submission of interesting cases for the website section 'Case of the Month'. All CoM submissions are eligible for selection for free registration at the next Euroson congress. Two cases that receive the most 'likes' in a year will receive free registration for the next EUROSON congress and the third most liked liked case will receive a cash prize of 100 EUR.
2022 Winners were:
Top rated is Sonographic Diagnosis of a Pott’s Puffy Tumor in a 5-year-old-girl - [Jul 2022]
M Brandt Department of Otorhinolaryngology, Head and Neck Surgery, University Hospital of Regensburg, Germany
Second is Ischemic Colitis as Complication of SARS-CoV-2 Infection - [June 2022]
Federica Lepore Department of Internal Medicine, San Matteo Hospital Foundation, University of Pavia, Italy
Both winners received free registration at EUROSON2023.
View Submission Template
Subclavian Steal Syndrome
Miguel Emilio Oliver Pece, Ultrasound Department, Hospital Virgen del Camino, Sanlúcar de Barrameda.

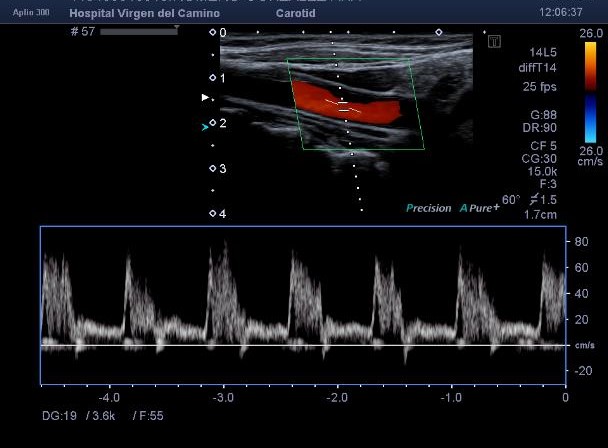



- An extensive plaque (Figure 1) in the left common carotid artery. However, there was no hemodynamic repercussion (Figure 2).
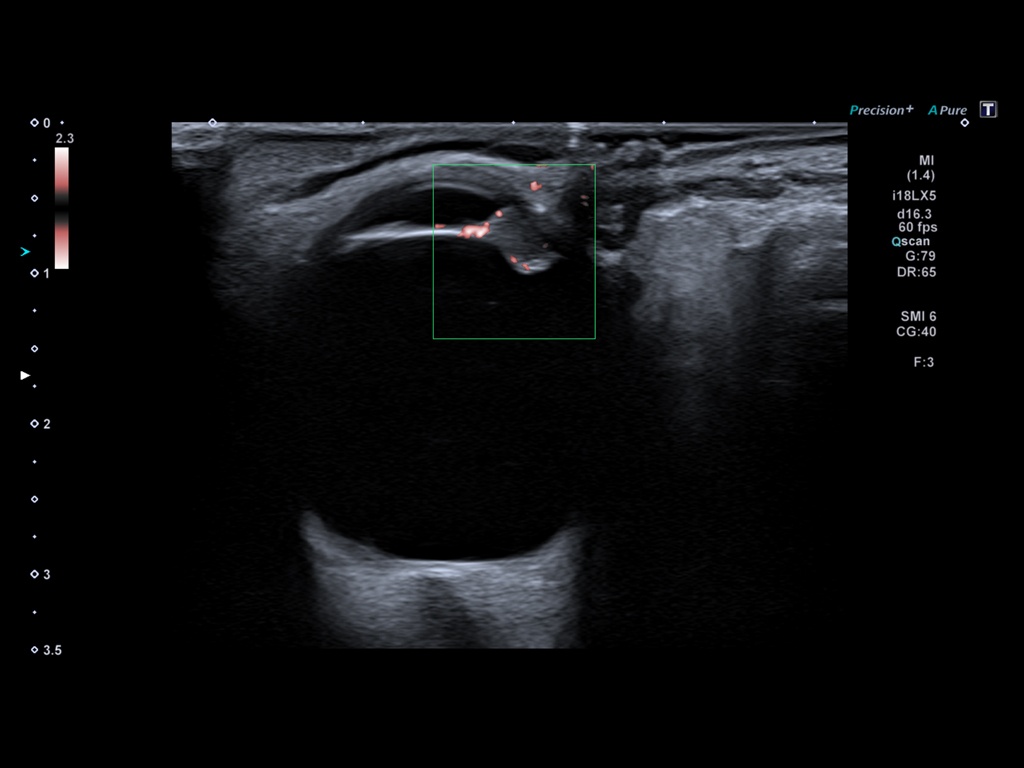
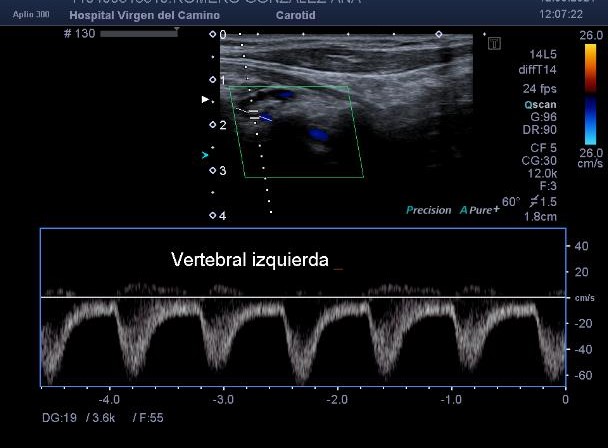
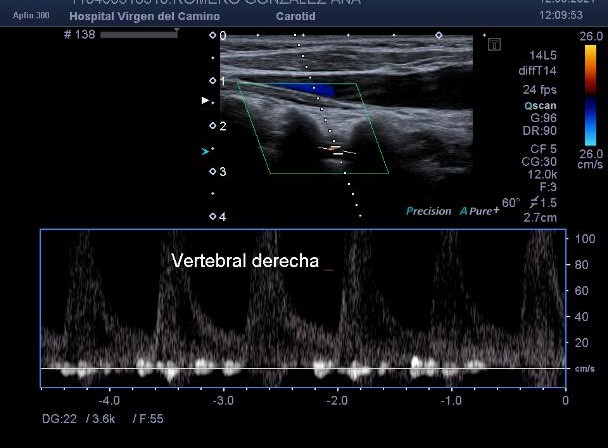
- Reversed flow in the left vertebral artery (Figure 3), both in systole and diastole.
- Increased peak systolic velocity in the right vertebral artery (Figure 4).
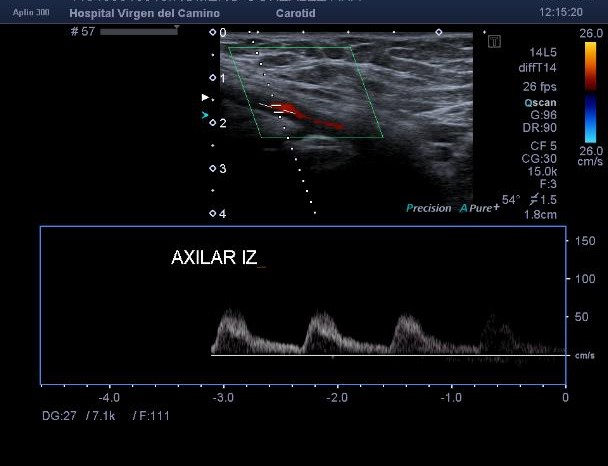
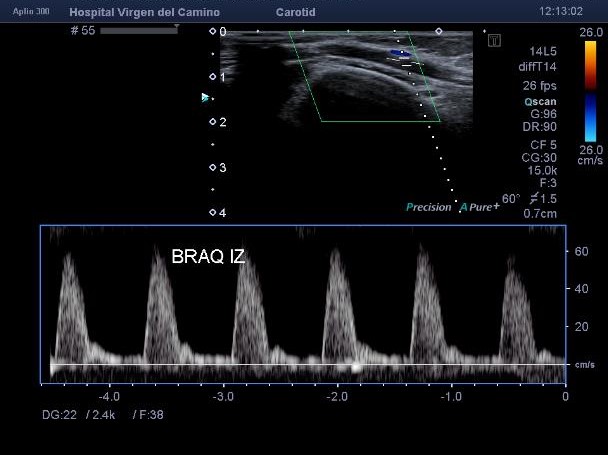
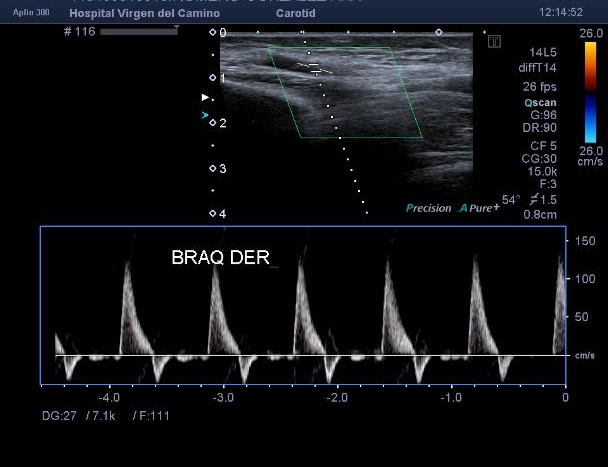
- Low resistance flow in the left subclavian, axillary and brachial arteries. (Figures 5, 6 and 7) and high resistencia flow in contralateral brachial artery (Figure 8)
CT angiography of supra-aortic trunks showed:
- Critical stenosis at the origin of the left subclavian artery. (Figure 9).
- Stenosis at the origin of the left vertebral artery. (Figure 10).
- No other relevant alterations in the rest of the supra-aortic trunks.
Subclavian steal syndrome (SSS) is a proximal subclavian artery stenosis, mainly due to atheromatous plaque formation, causing retrograde flow in the ipsilateral vertebral artery. It is accompanied by transient neurological symptoms secondary to ischemia of the affected territory. The prevalence is between 0.6% and 6.4% in the general population, with a male-to- female ratio of 2:1. The left subclavian artery is more frequently affected with a ratio of 4:1. Intermittent or partial steal occurs when the stenosis is between 60% and 90% and is manifested by bidirectional flow: anterograde in systole and retrograde in diastole.
CLINICAL PERSPECTIVE:
From a clinical perspective, SSS is typically characterized by symptoms such as arm pain, weakness, numbness, and dizziness, which result from a reversal of blood flow in the subclavian artery due to a blockage or stenosis. Other symptoms may include headache, vertigo, and syncope.
Physical examination may reveal reduced or absent pulses in the affected arm, and blood pressure measurements may show a significant difference between the two arms. Diagnostic testing such as Doppler ultrasound, CT angiography, or magnetic resonance angiography may be used to confirm the diagnosis and identify the location and extent of the blockage.
THERAPY PLANNING:
Treatment options for subclavian steal syndrome include medications (antiplatelets), lifestyle changes (quitting smoking), angioplasty, stenting, and surgery. The choice of treatment depends on various factors such as the severity of symptoms, the location and degree of stenosis, and the patient's overall health status. Follow-up care for patients with subclavian steal syndrome typically involves regular monitoring of symptoms and blood pressure, as well as surveillance imaging to detect any recurrence or progression of the blockage.
Treatment goals are to restore anterograde flow, relieve cerebral hypoperfusion and its symptoms, and improve perfusion of the affected limb.
OUTCOME & PROGNOSIS:
The patient was evaluated by Vascular Surgery department at the referral hospital. The following treatment wad indicated: 100 mg AAS daily, 20 mg simvastatin daily, follow-up with doppler ultrasound after one year and quit smoking. Surgical treatment was not considered necessary.
The prognosis of subclavian steal syndrome depends on various factors, including the severity and location of the blockage, the degree of collateral circulation, and the presence of any underlying medical conditions. In general, the prognosis is favorable for patients with mild or moderate symptoms, as these can often be managed effectively with medications and lifestyle changes.However, patients with severe symptoms or those who have developed complications such as stroke or heart attack may have a worse prognosis. The risk of these complications increases with the extent and duration of the blockage, and prompt intervention is therefore important to prevent further damage.
The choice of treatment also affects the prognosis, with some interventions such as angioplasty and stenting having a higher success rate and lower risk of complications compared to surgery. Overall, the prognosis of subclavian steal syndrome is generally good with appropriate management, although the presence of other risk factors such as diabetes, hypertension, and smoking can worsen the prognosis.
2) Lacey KO. Subclavian steal syndrome: a review. J Vasc Nurs. 1996 ;14(1):1-7.
3) Potter BJ, Pinto DS. Subclavian steal syndrome. Circulation. 2014;129(22):2320-3.
4) Komatsubara I, Kondo J, Akiyama M, et al. Subclavian steal syndrome: a case report and review of advances in diagnostic and treatment approaches. Cardiovasc Revasc Med. 2016;17(1):54-8.
5) Salenius JP, Uurto I. Subclavian steal -oireyhtymä [Subclavian steal syndrome]. Duodecim. 2011;127(20):2148-54..

{kind=link}